
Abstract
Objective. To define the clinical, serological, and histopathological characteristics of primary (pSS) and secondary Sjögren’s syndrome (SS).
Methods. Fifty subjects with pSS and 300 with connective tissue diseases (CTD; systemic lupus erythematosus 100, rheumatoid arthritis 100, scleroderma 100) were selected randomly from our patient registry. Selected patients were assessed for fulfillment of the American-European Consensus Group criteria for SS using a 3-phase approach: screening (European questionnaire, Schirmer-I test, wafer test), confirmatory (fluorescein staining test, nonstimulated whole salivary flow, anti-Ro/La antibodies), and lip biopsy (H&E and immunohistochemical staining for anti-CD20 and anti-CD45RO scored by morphometry).
Results. All patients with pSS and 65 with CTD met criteria for SS. Oral symptoms (pSS = 92% and secondary SS = 84%; p = 0.02), parotid enlargement (pSS 56%, secondary SS 9.2%; p < 0.001), and higher prevalence (pSS 82%, secondary SS 41%; p < 0.001) and titers of anti-Ro/La antibodies were more common in pSS. Extraglandular manifestations were similar in both groups, except for Raynaud’s phenomenon, which was more common in those with secondary SS (pSS 16% vs secondary SS 41%; p = 0.001). These results remained after 3 different sensitivity analyses. The prevalence of focal infiltration was also similar in both SS varieties; however, a higher B:T cell ratio and higher expression of CD20 cells (2922 vs 607.5 positive cells; p < 0.001) were observed in pSS.
Conclusion. A higher frequency of oral symptoms and parotid enlargement and stronger B cell activity (autoantibody production and lymphocyte infiltration) were observed in pSS. Whether these results reflect a true difference between the 2 disease entities or derive from underlying variables remains uncertain.
- SJÖGREN’S SYNDROME
- FOCAL SALIVARY INFILTRATION
- EPIDEMIOLOGY
Sjögren’s syndrome (SS) is an autoimmune disorder affecting primarily the exocrine glands, leading to keratoconjunctivitis sicca and xerostomia1, but it can also include extraglandular features2. SS is classified as primary (pSS) when the clinical manifestations occur alone, or as secondary (sSS) when associated with another autoimmune disease, usually a connective tissue disease (CTD)3. Classification criteria for both entities have been proposed by the American-European Consensus Group (AECG)4, the main difference being that anti-Ro/La antibodies are not a criterion for sSS.
The prevalence of sSS has been reported to be from 4% to 31%5–14, depending on the criteria applied4,15,16, the methodological design, and the associated CTD. Among patients with rheumatoid arthritis (RA) the prevalence ranges between 4% and 31%5–7, in systemic lupus erythematosus (SLE) between 8% and 19%8–10, and in scleroderma between 14% and 29%11–14. In our institution, the prevalence of sSS is 19.3%17.
Despite being a frequent disorder, sSS has not been studied extensively. Moreover, there is uncertainty whether sSS is merely a manifestation of the underlying disease or a true overlap of pSS with another CTD. Studies to date have compared patients with a specific CTD and SS to patients with pSS to evaluate whether these 2 entities are indeed different. Manoussakis, et al9 found that in comparison with pSS, patients with SLE and SS were younger, but had similar clinical, serological, and histological features, with the exception of perivascular infiltrates in the salivary gland biopsies, suggesting that pSS and sSS are the same entity. Recently, a study18 found that subjects with sSS in the setting of scleroderma had frequencies of xerostomia, dry eye symptoms, positivity for anti-Ro/La antibodies, and classic histological pattern similar to those of subjects with pSS, again suggesting that these 2 entities are the same. Conversely, patients with RA and sSS are more frequently asymptomatic and have a lower prevalence of parotid gland enlargement5 than subjects with pSS.
We compared the clinical, serological, and histopathological characteristics between patients with pSS and patients with diverse CTD and SS. All subjects were randomly selected from a large population of patients with various CTD and in whom SS was established using a structured approach, and defined according to the AECG criteria4, in order to determine whether the 2 entities are or are not the same.
MATERIALS AND METHODS
Patients
The study was conducted in a tertiary care center, where the rheumatology clinic provides regular care to 5942 patients, of whom 4813 (81%) have CTD. Using random numbers, 50 out of 81 patients with primary SS, 100 of 2527 with RA, 100 of 1860 with SLE, and 100 of 136 with scleroderma were selected from our patient registry, and assessed for SS criteria4 using a structured approach. Considering the medical literature and results of our previous study17, the prevalence of SS is around 20% in patients with CTD; thus 300 patients with CTD would provide us with a similar number of subjects with sSS to enable a robust comparison with the pSS group.
To be eligible, patients had to meet classification criteria for their CTD19–21, to take no medication that would reduce salivary flow (i.e., antihistamines, sedatives, beta-blockers, diuretics, etc.) within 48 hours before the study, and to have no history of hepatitis C or HIV infection, sarcoidosis, lymphoma, or graft versus host disease or a history of neck/head radiotherapy.
We obtained approval for the study from the Institutional Biomedical Research Board and all patients gave signed informed consent to participate according to the Declaration of Helsinki.
Confirmation of Sjögren’s syndrome
All participating patients were subjected to a standardized evaluation, designed in 3 phases: screening, confirmatory tests, and lip biopsy, to assess the presence of SS according to the AECG criteria4.
Participants were asked to refrain from eating, drinking, smoking, chewing, or oral hygiene procedures for at least 1 hour before the evaluation, and were seen in a closed room with no air-conditioning or heating, during the morning. The presence of extraglandular manifestations ever was assessed from subjects’ medical records and by direct questions during the interview.
Screening phase
All patients had a face-to-face interview with a single rheumatologist, using a standardized form that included questions about demographic data and use of medications. In addition, a validated 6-item screening questionnaire for oral and ocular sicca symptoms4 was applied and the Schirmer-I test4 and the wafer test22 were carried out.
The Schirmer-I test was done using 2 standardized sterile tear measurement strips (Tear Flo; Rose Stone Enterprises, Alta Loma, CA, USA), and the wafer test was done as described22. Patients with at least one affirmative response to the screening questionnaire, Schirmer-I test ≤ 5 mm in 5 minutes, or wafer test > 4 minutes were considered to have a positive screening.
Confirmatory phase
Patients with positive screening underwent this phase, consisting of fluorescein staining test, nonstimulated whole salivary flow rate (NSWSF), and testing for autoantibodies (anti-Ro/La) by ELISA (The Binding Site, Birmingham, UK). The fluorescein staining test was performed by 2 ophthalmologists blinded to the patients’ diagnosis. Each evaluated roughly 50% of the total population. The test was considered positive with a score ≥ 4 according to the Bijsterveld scale in at least one eye4.
NSWSF collection was performed as reported23. Saliva was collected during 5 minutes and volume expressed as ml/5 min. The confirmatory phase was also performed in a random sample of 10% of patients with negative screening.
Lip biopsy
Lip biopsy was proposed for all patients who had > 2 of the following results: (1) at least one affirmative answer to the oral component of the screening questionnaire; (2) wafer test > 4 min; (3) presence of keratitis by fluorescein staining test; (4) NSWSF < 1.5 ml/5 min; and (5) positive anti-Ro/La antibodies.
Biopsies were discarded if no gland tissue was obtained. An expert pathologist (CAC) evaluated all biopsies blinded to clinical data. Light microscopy examination was carried out on hematoxylin and eosin (H&E) staining at 4× magnification. Histological evaluation focused on the presence of lymphoid infiltrate. Focal lymphocytic sialoadenitis was diagnosed based on a focal score of one or more lymphocytic foci (> 50 lymphocytes per 4 mm2)4.
For immunohistochemical techniques, tissues were fixed in 4% paraformaldehyde and embedded in paraffin. Sections were incubated with anti-CD45RO and anti-CD20 antibodies (Dako, Palo Alto, CA, USA) at 1:10 dilution. CD45RO+ lymphocytes were antigen-primed/memory T lymphocytes and CD20+ cells were B lymphocytes. The immunoreactivity signal of these antibodies was detected with a streptavidin-biotin peroxidase reaction (LSAB+ kit; Dako) and visualized by exposure to diaminobenzidine. Twenty-five to 35 consecutive non-crossed fields (4.68 × 6.36 mm at 20× magnification) per biopsy were photographed by light microscopy. Only 25 fields were quantified for antibody expression and recorded with a digital video camera (CoolSnap Pro, Media Cibernetics, Silver Spring, MD, USA). Pictures were processed on a computer and evaluated by morphometric analysis using Image-Pro 5.1 (Media Cybernetics) and Photoshop 7 (Adobe Systems, San Jose, CA, USA)24. Taking advantage of the color recognition capabilities of this software, brown positive-staining areas were selected and quantified in the number of positive cells. For each field examined, the number of positive areas was expressed as the number of positive cells of the total area of each evaluated field. Finally, for each biopsy, brown background staining was extracted for the measurement; in order to be more specific, the color range of the histogram was reduced for every measurement.
Statistical analysis
Patients with pSS and sSS were classified according to the diagnostic criteria for each SS variety4. The clinical (glandular and extraglandular), serological (anti-Ro/La antibodies), and histopathological characteristics were compared between the 2 patient groups.
Categorical variables were compared by chi-square or Fisher’s exact test when appropriate; continuous variables were compared using Student’s T test or Mann-Whitney U test. Prevalence estimates were reported with 95% confidence intervals. Two-tailed p < 0.05 was considered significant. All analyses were performed using SPSS for Windows 15.0 (SPSS Inc., Chicago, IL, USA).
Sensitivity analyses
We compared the pSS group to each subgroup of sSS according to the concomitant CTD. We also assessed for differences among the subgroups of sSS according to the CTD. In addition, since pSS criteria consider the presence of anti-Ro/La antibodies, while the criteria for sSS do not, we also performed an analysis applying the pSS criteria to identify patients with SS in the CTD groups. For the same reason, as a different prevalence of anti-Ro/La antibodies was expected in pSS and sSS, we also performed an analysis including patients in whom pSS diagnosis was based on the lip biopsy.
RESULTS
From the 350 original randomly selected participants, 115 (33%) did not participate in the study (54 not located, 34 declined to participate, 16 failed to meet ACR criteria19–21, 8 had hepatitis C, 1 had HIV infection, and 2 were dead). These patients were replaced by new randomly selected subjects from the same registry to achieve the planned study sample.
The originally selected patients and the final study population were similar for age and sex. The mean age of the rheumatology registry population, 56.6 ± 11.5 years and 46.3 ± 15.1 years for patients with pSS and CTD, respectively, was similar to the final study group. However, the percentage of men with SLE was higher in the rheumatology registry (7.5%) than in the study sample (4%).
The majority of the study population consisted of women. Patients with pSS were older than the patients with CTD (56.0 ± 11 yrs vs 47.8 ± 15 yrs, respectively; p < 0.001), but the mean disease duration was similar between groups. Patients with pSS were receiving prednisone and immunosuppressants less often than patients with CTD (p < 0.001). Table 1 shows the general characteristics of the study population.
Characteristics of the study population.
Process of patients through the study. Screening phase
Screening was positive for all patients with pSS. In the CTD group, at least one affirmative answer in the ocular or the oral sections of the screening questionnaire was given for 112 (37%) and 94 (31%) patients, respectively. The Schirmer-I test was positive in 145 (48%) patients, and the wafer test in 201 (67%). Thus, screening was positive for 250 patients (83%) with CTD (89% with RA, 70% with SLE, 91% with scleroderma) and these patients advanced to the confirmatory phase. Results for each disease are shown in Table 2.
Results of the 3-phase assessment.
Confirmatory phase
Most patients with pSS had low salivary flow and tested positive for anti Ro/La antibodies; however, only half of them had an abnormal fluorescein test. Among the 250 subjects with CTD who qualified for this phase, NSWSF was abnormal in 168 (67%), the fluorescein staining test was positive in 106 (45%), and anti-Ro/La antibodies were positive in 67 (27%) patients (Table 2).
Among 10 randomly selected patients with CTD and negative screening in whom confirmatory tests were carried out, none required lip biopsy.
Lip biopsy
All patients in the pSS group and 201 in the CTD group met criteria for lip biopsy. In the pSS group, biopsy was performed in half of the patients; among the 25 patients who declined the biopsy, 2 had a previous diagnostic biopsy, and the remaining patients met SS criteria because they tested positive for anti Ro/La antibodies. In the CTD group, lip biopsy was performed in 82 (41%) patients, 103 declined it, and 16 had a contraindication (anticoagulation therapy in 14 cases and severe thrombocytopenia in 2 patients). Despite the lack of biopsies in 119 eligible subjects, we were able to determine the SS status with the remaining classification criteria in 88 patients, but in 31 patients the lip biopsy result was decisive for the diagnosis.
Prevalence of SS in patients with CTD
Sixty-five of the 300 patients with CTD met criteria for sSS, for prevalence of 21.7% (95% CI 17%–25%). In 204 patients sSS was ruled out, and in 31 patients (10.3%) it was undefined. Therefore, the minimum prevalence of SS by CTD was as follows: RA 20% (95% CI 13%–27%), SLE 15% (95% CI 9%–21%), and scleroderma 30% (95% CI 22%–38%).
Clinical and serological characteristics of primary and secondary SS
The diagnosis was confirmed according to the AECG criteria among the 50 patients from the pSS group, and sSS was identified in 65 patients with CTD. Patients with pSS and sSS were comparable for age, sex, and most of the ocular features; however in pSS a higher prevalence of oral symptoms (98% vs 85% in sSS; p = 0.02) and parotid enlargement (56% vs 9% in sSS; p < 0.001) was observed.
Subjects with pSS were more frequently positive for anti-Ro/La antibodies (82% vs 41%; p < 0.001), and also had higher titers of the antibodies (p < 0.001), than patients with sSS. The levels for anti-Ro were 890 (1.3–57,700) U/ml and 4 (1.2–36,900) U/ml in pSS and sSS, respectively; and for anti-La 7.5 (4.3–13,620) U/ml and 4.9 (2.1–146,300) U/ml, respectively. Nevertheless, the prevalence of anti-Ro/anti-La antibodies was greater among patients with sSS (41%) compared to the overall CTD population (27%) (p = 0.001).
Extraglandular manifestations were similar in the 2 groups, except for Raynaud’s phenomenon, which was more common in sSS (41% vs 16% in pSS; p = 0.001). Also, the use of immunosuppressants and prednisone was more common in sSS (p = 0.002 for each; Table 3).
Characteristics of patients with primary and secondary Sjögren’s syndrome.
Histological and immunohistochemical analyses
Overall, 107 lip biopsies were performed (25 in the pSS and 82 in the CTD group); 4 biopsies were discarded (one pSS and 3 from the CTD group); the remaining specimens contained a median of 4 glands (range 1 to 7). Among the 24 lip biopsies in the pSS group, 18 showed focal and 6 nonfocal lymphocytic infiltration. In patients with CTD, focal lymphocytic infiltration was seen in 44 biopsies, of which 27 patients met criteria for SS; nonfocal lymphocytic infiltration was observed in 33 biopsies, of which 9 patients met SS criteria, and 2 lip biopsies were normal. Forty-one biopsies, 17 with focal and 24 with nonfocal lymphocytic infiltration, corresponded to patients with CTD who did not meet criteria for SS. Thus, the prevalence of focal (75%) and nonfocal (25%) lymphocytic infiltrate in both varieties of SS was identical (Figure 1).
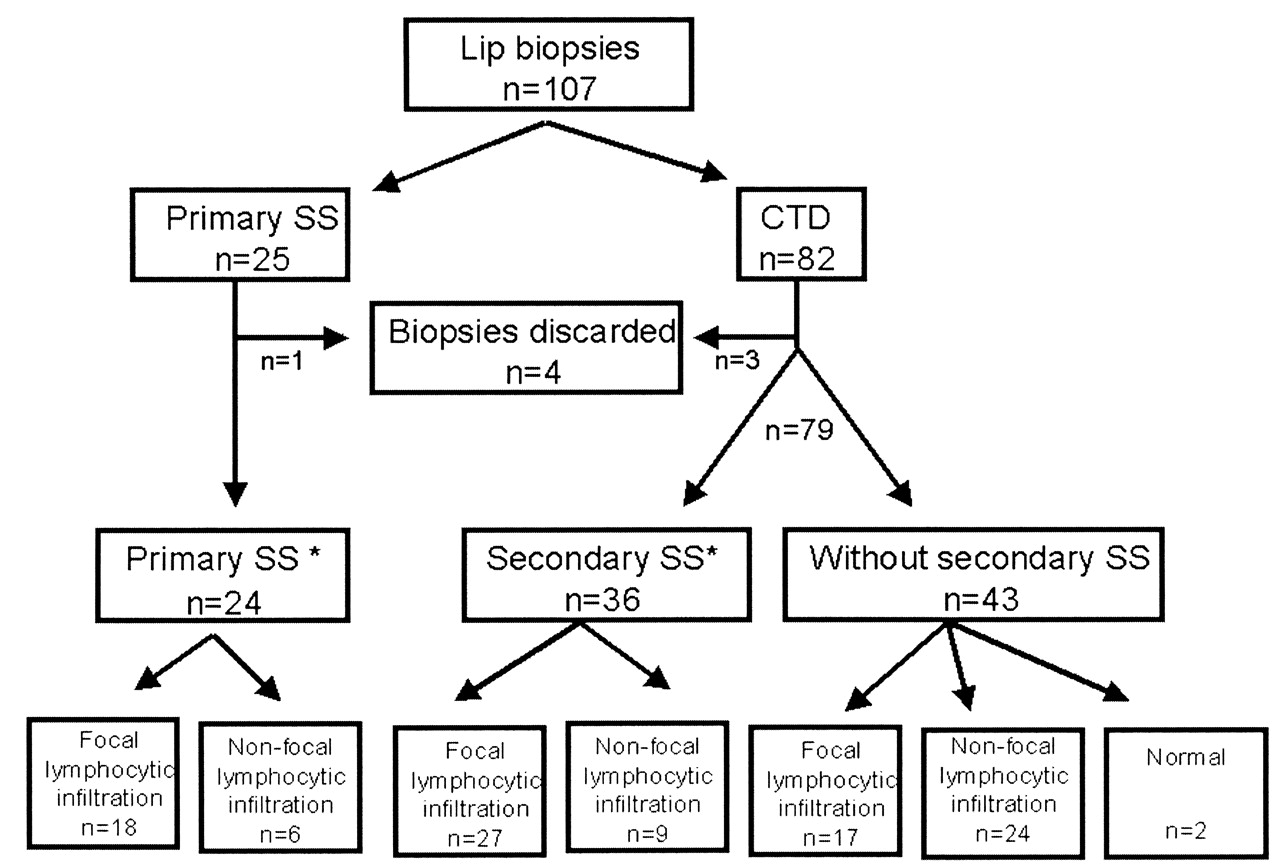
Classification of lip biopsy specimens. *Histological analysis for H&E staining.
Immunohistochemical staining for anti-CD20 and anti-CD45RO was performed in 75 specimens with adequate material (Table 4). In pSS, infiltrating lymphocytes displayed a stronger CD20-positive expression than CD45+RO expression (ratio 2:1). However, in sSS the CD20/CD45RO ratio was 0.46, and among CTD patients without SS the ratio was 0.70. Further, the expression of CD20 also predominated when comparing pSS and sSS biopsies (2922 vs 607 positive cells, respectively; p < 0.001; Figure 2). These results remained when biopsies with focal lymphocytic infiltration were analyzed, whereas no clear difference was observed in biopsies with nonfocal lymphocytic infiltration. Positive expression of CD20 tended to be stronger among patients with sSS than in CTD patients without SS, especially in those with focal lymphocytic infiltration; however, these differences were nonsignificant.

{kind=link}
{kind=link}
Minor salivary glands with focal lymphocytic infiltrates visualized by H&E stain and immunohistochemical staining for anti-CD20 and anti-CD45RO (4× original magnification). Images represent patients with primary SS (Line A), secondary SS (Line B), and connective tissue disease without SS (Line C).
Immunohistochemical staining results. Results are expressed as median (range) of positive cells.
No differences were observed in the expression of CD45RO cells in patients with pSS and those with sSS when either focal or nonfocal infiltrates were compared; however, the expression of CD45RO was stronger in both varieties of SS than in CTD patients without SS when all types of infiltration were analyzed.
Sensitivity analyses
Analysis of subgroups of sSS by CTD in comparison with pSS (Table 5) showed a younger population among SLE patients (p = 0.03). Again, the oral symptoms (except in SLE) and parotid enlargement predominated in the pSS population. Also, the prevalence and levels of anti-Ro and anti-La antibodies were significantly higher in pSS, with the exception of the titers of anti-La antibody in the setting of SLE. As expected, the frequency of extraglandular manifestations was related to the underlying CTD. Thus, Raynaud’s phenomenon in scleroderma as well as renal involvement and nonerosive arthritis were more prevalent in SLE. We found no differences among glandular and serologic features in the 3 subgroups of patients with sSS (data not shown).
Characteristics of secondary Sjögren’s syndrome by connective tissue disease in comparison with primary Sjögren’s syndrome.
When the pSS criteria were applied to the patients with CTD, 49 (16.3%) patients with SS were identified. These patients were younger (50 ± 11 yrs; p = 0.04) and had fewer ocular symptoms (69%; p < 0.004) than the pSS group, whereas parotid enlargement and oral manifestations continued to be more prevalent in pSS. All the other clinical, serological, and histological features with H&E staining remained unchanged (data not shown).
Finally, when we analyzed patients classified by the lip biopsy result, the differences in the prevalence and levels of anti-Ro/La antibodies among pSS and sSS still persisted (p < 0.001 for both comparisons).
DISCUSSION
We observed that patients with pSS had a higher frequency of oral symptoms, parotid enlargement, and presence and levels of anti-Ro/La autoantibodies, and a predominantly B type lymphocyte infiltration in the lip biopsy, in comparison to patients with sSS.
Study participants were randomly selected from a large population of patients with diverse CTD attending a tertiary care center. The presence of SS was assessed in each participant using a structured approach, and diagnosed according to the AECG criteria4. Selected patients with pSS and CTD were similar in age and sex to the total patient population with these diseases. Among the patients with CTD, the prevalence of SS was 21.6%, a result that falls within the range reported in ambulatory patients in our institute17 and in other studies5–14. Thus we consider that the ascertainment of SS was valid and unbiased and the study subjects were representative of our patient population.
Secondary SS has been recognized as an entity that generally follows the diagnosis of another CTD by 10 years on average25, but in some cases may precede it26. Some investigators describe it as “secondary,” others as “associated”9,18,27, implying 2 concepts: being part of the spectrum of the underlying CTD or being a true overlap syndrome. Thus, there is debate whether pSS and sSS represent the same entity or not.
Two studies have explored the characteristics of sSS in smaller samples of patients with SLE and scleroderma, and they found no differences in clinical, serological, and histopathological characteristics compared to a pSS population9,18. Conversely, we observed that parotid gland enlargement and oral symptoms were more frequent in patients with pSS, whereas the rest of the glandular manifestations were alike in both SS categories. Overall, extraglandular manifestations were also similar in both groups, except Raynaud’s phenomenon, which occurred more commonly in sSS. A previous study reported a higher prevalence of peripheral neuropathy in patients with scleroderma and SS than in those with pSS18.
Contradictory information about the prevalence of anti-Ro/anti-La antibodies has been published. Some studies report a similar frequency of anti-Ro/La antibodies in patients with pSS, SLE with SS9, and scleroderma with SS18. On the other hand, another study found a higher prevalence and titers of anti-Ro/La autoantibodies in SLE patients with SS27. In agreement with a study of 62 patients with pSS and 28 with sSS28, we found an increased prevalence and levels of anti-Ro/La antibodies in the primary variety. Our results persisted after the sensitivity analyses, with the exception of the levels of anti-La antibodies that were similar in pSS and patients with SLE and sSS.
It is notable that we observed a greater prevalence of anti-Ro/La antibodies in primary and secondary SS than previous studies2,5,9,18; although we have no clear explanation for these results, we do not consider that this reflects selection bias, since participants were randomly selected and autoantibody testing was done by protocol in all the participants, thus we consider this the only possible explanation of these results. Proof of this is that the prevalence of anti-Ro/La antibodies among the SLE patients, regardless of SS status, was 32%, which is similar to the prevalence reported elsewhere29.
Chronic focal periductal lymphocytic sialoadenitis is the hallmark of pSS30,31. In our study, the prevalence of focal lymphocytic infiltration was as common in pSS as in sSS, findings consistent with previous reports9,18. An interesting finding was that 17 patients with CTD showing focal lymphocytic infiltration did not meet the criteria for SS. Whether these patients present an early or preclinical stage of SS requires further analysis, perhaps based on genetic studies and a longer followup.
Based on the immunohistochemistry analysis, we detected in pSS subjects that infiltrating lymphocytes displayed a major positive CD20 expression compared to CD45+RO; however, in sSS and among CTD patients without SS this ratio was < 1. These results persisted in biopsies with focal lymphocytic infiltration, whereas no clear difference was observed with nonfocal lymphocytic infiltration. Our results are consistent with a report where the major portion of mononuclear cells infiltrating pSS salivary glands were B lymphocytes32. In early-stage disease, a predominance of primed CD4+ (CD45RO+) T cells in minor salivary gland infiltrate is observed, whereas B cells comprise about 20% of the infiltrate33. Lymphocytic sialoadenitis in pSS is thought to be a stepwise process, thus higher degrees of lymphoid organization are associated with progressive increases in the proportion of B cells. Overall these results reflect B cell hyperactivity in pSS33. The finding that B lymphocytic infiltration in pSS is stronger than in the secondary variety suggests that these entities may have different physiopathology and different prognosis. In the same way the risk for developing lymphoproliferative disorders in pSS rather than sSS is well known34,35.
At first examination, these differences might suggest that pSS and sSS are different entities; nevertheless the following variables between the 2 patient populations need to be considered as alternative explanations: (1) A potential referral bias may be present, since patients with pSS attending a tertiary care center may have more severe disease. Also, ascertainment bias cannot be excluded, because in patients with CTD the presence of SS may be suspected and evaluated at an earlier stage. (2) Most patients with CTD were receiving prednisone and immunosuppressants, in comparison with less than one-third of pSS patients. Consideration is needed of whether immunosuppressants may modify the clinical spectrum, the presence and levels of autoantibodies, or the inflammatory infiltrate in salivary glands. (3) Forty-five out of 65 patients with sSS had scleroderma or SLE, diseases where Raynaud’s phenomenon is common. Thus, the clinical expression of these diseases may explain the difference observed with pSS.
Other potential limitations of our study: (1) A third of the patients originally selected declined to participate. Although they were replaced by patients from the same source population using random numbers, it could not be established whether their decision to participate was related to the presence of SS. (2) It was not possible to perform lip biopsies in all the patients who met criteria because they rejected the procedure or there was contraindication for it. Although the effect of this on defining the status of sSS was minimal, we do not know if a larger number of biopsies would have modified the histopathological features. (3) In addition, our SS prevalence in those with scleroderma may be an overestimation due to patients with sicca symptoms or signs in whom this may be due to fibrosis rather than lymphocytic infiltrate; this could not be determined without a lip biopsy; however, those patients actually met the criteria for SS. In our study 15 (50%) patients with scleroderma and SS did not have a biopsy — but the other patients with lip biopsy did show lymphocytic infiltrate, not fibrosis. These patients met the SS criteria, even if a lip biopsy result were not considered. We believe this illustrates a weakness of the current classification criteria, thus we conducted several sensitivity analyses in order to overcome such potential limitations.
Major strengths of our study include that the population evaluated derives from a very large number of patients with diverse CTD. All patients had the same probability to participate in the study and all the selected patients were evaluated identically to determine SS status. Therefore we consider that the results are reliable. Since the population of patients with sSS consisted of individuals with 3 different CTD, we had a more robust clinical scenario for sSS for comparison with the primary variety than those studies where patients with sSS derive from a single-CTD group.
In summary, patients with pSS had a higher frequency of oral symptoms and parotid enlargement, higher prevalence and levels of anti-Ro/anti-La autoantibodies, and a predominantly B type lymphocyte infiltration in the lip biopsy. Whether these results establish that primary and secondary Sjögren’s syndrome are 2 different entities, or whether the clinical spectrum of Sjögren’s syndrome simply varies due to underlying variables such as immunosuppressive therapy, could not be determined conclusively. The study of other features such as genetic backgrounds might resolve this controversy.
Footnotes
-
Supported by the Consejo Nacional de Ciencia y Tecnología de México 81920.
- Accepted for publication November 19, 2009.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.