
Abstract
Objective. To conduct a retrospective study to assess whether the degree of thumb involvement differs between primary Raynaud’s phenomenon (PRP) and secondary Raynaud’s phenomenon (SRP).
Methods. Thermography images from all patients attending Salford Royal Hospital and referred for thermography for assessment of RP between 2004 and 2006 were retrospectively reviewed. A distal dorsal difference (DDD) of −1°C or less between the fingertips and dorsum of the hand (fingers cooler) at 23°C was considered clinically relevant. The worse score (the lower score, i.e., the more negative value) from each pair of digits was considered for analysis.
Results. One hundred seventy patients fulfilled the study criteria. DDD at 23°C for the thumbs were significantly higher (digital tips warmer) compared with other digits (p < 0.001) in both PRP and SRP. All digits were significantly warmer in PRP compared to SRP with the exception of the thumbs. The proportion of patients with clinically relevant involvement of thumbs was significantly higher in SRP compared to PRP (p = 0.003) and this difference was more pronounced in the thumbs compared with other digits.
Conclusion. Although the median temperature gradient along the thumb was not significantly different between SRP and PRP, the thumb is more likely to be involved in SRP than in PRP. Thumb involvement is one of a number of clinical indicators that should alert the clinician to the possibility of an underlying connective tissue disease/disorder.
- RAYNAUD’S PHENOMENON
- THUMB SPARING
- THERMOGRAPHY
- SYSTEMIC SCLEROSIS
- CONNECTIVE TISSUE DISEASES
Raynaud’s phenomenon (RP) is classically characterized by triphasic color changes in response to cold or emotional stress. RP can be divided into primary (PRP) and secondary RP (SRP) depending on the absence or presence of an underlying disorder, e.g., a connective tissue disease (CTD) such as systemic sclerosis (SSc)1. Complete reversibility of episodic digital ischemia is an important characteristic of PRP and is a distinguishing feature from SRP in which irreversible tissue damage can occur.
In a prospective study2 we demonstrated that the thumb is spared in both PRP and SRP, as evidenced by patients’ self-reported symptoms (subjective assessment) and thermography (objective assessment). On thermography, the thumb distal-dorsal difference (DDD) scores (measuring the temperature difference between the digital tip and the dorsum of the hand at 23°C) were better, i.e., higher in PRP compared with SRP; however, there was no evidence that the degree of thumb-sparing was different between the PRP and SRP groups. We concluded that the sample size lacked enough power to answer this question. It is important to know whether the thumb is more involved in SRP compared to PRP; if so, this could point to an underlying CTD and this could help rheumatologists categorize patients. In this retrospective study we identified a large sample of patients with RP to determine whether the degree of thumb involvement differs between PRP and SRP.
MATERIALS AND METHODS
Patients
Patients were identified retrospectively on the basis that (1) they had undergone thermography at Salford Royal Hospital between 2004 and 2006; and (2) they satisfied our criteria for RP (at least one color change; white, blue, or red in response to cold as documented by the attending physician). Case notes were reviewed (electronic and/or paper) and patients were subdivided into those with PRP and with SRP. Patients with PRP satisfied the LeRoy and Medsger criteria1. Patients with SRP had either an identifiable underlying disorder (Table 1) or undifferentiated connective tissue disease (UCTD). All patients with UCTD were positive for anti-nuclear antibodies (ANA; positivity defined by IgG titer ≥ 1/100). Some had positive antibodies to extractable nuclear antigens and some had abnormalities on nailfold microscopy.
Demographic and clinical details of all patients.
The study was approved by the Warrington, Wigan and Leigh Research Ethics Committee.
Thermography protocol
Thermography images were retrieved from the vascular laboratory database at Salford Royal Hospital. Thermography was performed by senior vascular technicians using a standard protocol. An Agema 570 infrared thermography camera (Flir Systems Ltd., West Malling, UK) and the Agema Research 2.1 software were used. Patients were asked to refrain from caffeine/nicotine for 4 h prior to testing. After acclimatization at 23°C for 20 min in a temperature controlled room an image of the dorsum of each hand was taken, and from these hand images the DDD was calculated, i.e., the temperature of the tip of the fingers minus the temperature of the dorsum of the hand. A DDD of −1°C or less at 23°C was prespecified to be considered clinically relevant involvement3,4. The worse score (the lower score, i.e., the more negative value) from each pair of digits (right or left hand) was considered for analysis.
Sample size
Assuming there would be double the number of cases with SRP as PRP, it was calculated that 48 patients with PRP and 96 with SRP would allow detection of a difference of 0.5 SD in the outcome (i.e., the average temperature gradient along the thumbs) with 80% power. We identified 67 patients with PRP and 103 with SRP, giving 88% power.
Statistical analysis
The results were analyzed using repeated-measures analyses of variance (ANOVA), independent samples t tests, and chi-square tests in SPSS version 16.
RESULTS
Patients
Demographic details of the 170 patients whose thermography results were included are summarized in Table 1. The median age of patients was 46 years (range 18–78 yrs). Sixty-seven (52 women, 15 men) had PRP and 103 (84 women, 19 men) had SRP. Patients with SRP were older than patients with PRP. Forty-seven (41 women, 6 men) had SSc. Thirty-nine patients (30 women, 9 men) who had SRP but did not have a specific CTD were classified as having a UCTD. All patients classified as UCTD were ANA-positive. Details of other disorders are summarized in Table 1. Fifty-seven patients (33%) were receiving vasoactive drugs such as calcium-channel blockers and angiotensin-converting enzyme inhibitors. Of the 57 patients who were taking vasoactive drugs, 8 (14%) fulfilled the criteria for PRP and 49 (86%) SRP.
Thermography results
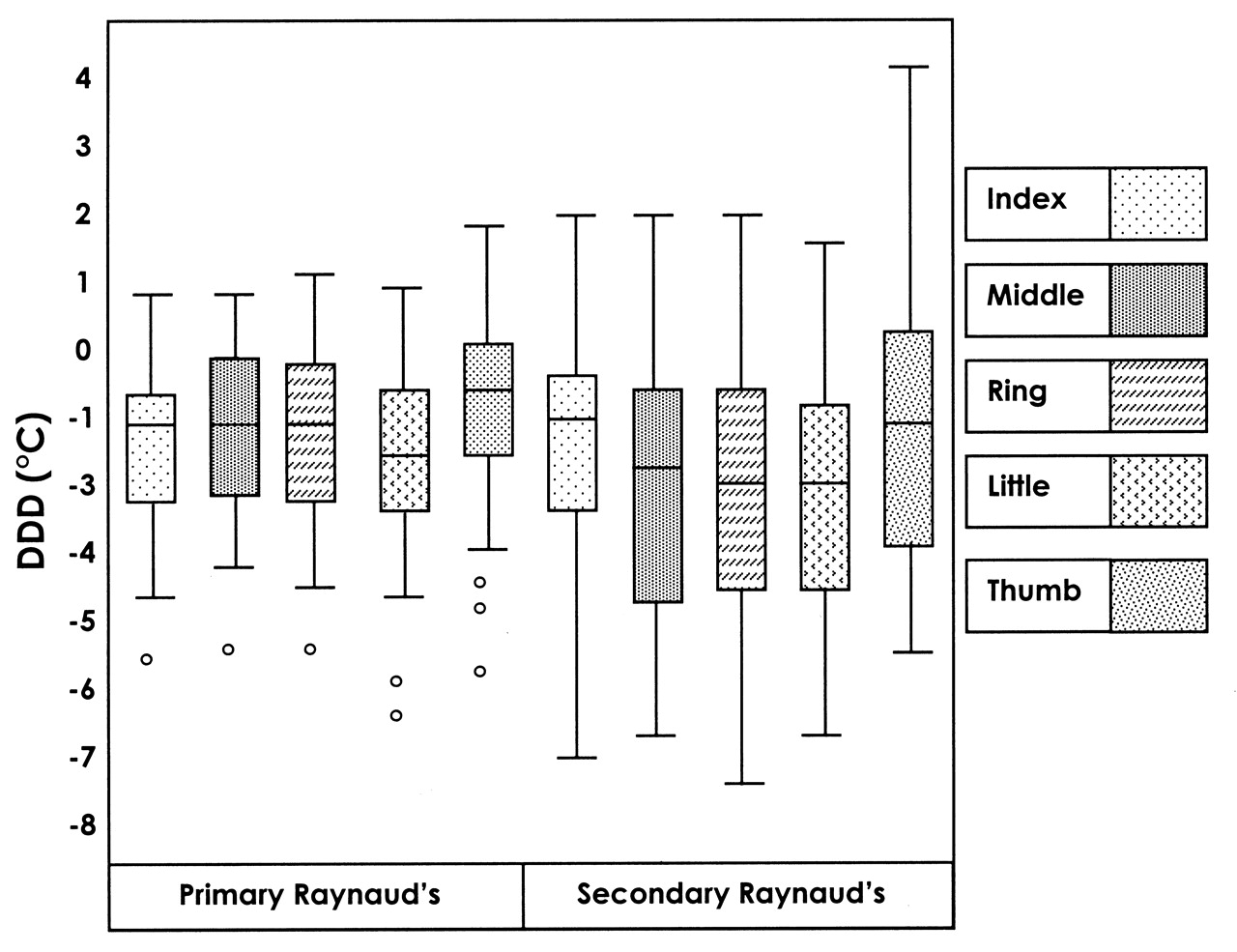
The thumbs were significantly warmer compared to other digits in both PRP and SRP, i.e., the DDD at 23°C for the thumbs were significantly higher compared with other digits (p < 0.001; Figure 1). Comparison of the DDD at 23°C of each digit between PRP and SRP showed all digits were significantly warmer in PRP compared to SRP, with the exception of the thumbs, which were of borderline significance (p = 0.07; Figure 1, Table 2). This could be due to the degree of thumb-sparing being more pronounced in SRP compared with PRP. The proportion of patients with clinically relevant DDD (DDD at 23°C of −1°C or less) in thumbs was significantly higher in SRP compared to PRP (p = 0.003; Table 3). This difference in the proportion of patients (PRP vs SRP) with a clinically relevant DDD was more pronounced in the thumbs than in other digits (Table 3).
{kind=link}
The distribution of worse distal dorsal difference (DDD) scores of each pair of digits, allowing comparison between the thumb and other digits and comparison between primary RP (n = 67) and secondary RP (n = 103). Upper and lower ends of whiskers represent highest and lowest values, respectively; upper and lower ends of the box represent 75th and 25th centiles; horizontal line represents the median score; circles represent outliers.
Comparison of mean distal dorsal differences at 23°C for each digit between primary RP and secondary RP.
Comparison of clinically relevant distal dorsal differences at 23°C for each digit between primary RP and secondary RP.
DISCUSSION
This is the first study to show that the degree of thumb involvement differs between PRP and SRP. We found significantly greater involvement of the thumb in SRP compared with PRP as evidenced by a significantly higher proportion of patients who had clinically relevant DDD at 23°C. A DDD of −1°C or less (dorsum warmer than the tip of fingers) was taken as clinically relevant3,4, as in our previous study2.
It was not the purpose of our study to distinguish PRP from SRP. However, although not conclusive, thumb involvement should alert rheumatologists to search for an underlying CTD. Other features of RP that should alert a rheumatologist to the possibility of an underlying CTD include disease onset at age > 30 years, severe episodes, asymmetrical involvement, digital ulcerations/necrosis, abnormal nailfold capillaries, and positive serology such as ANA5. Some features are better predictors for development of CTD than others; for example, abnormal nailfold capillaries in a patient with RP are a better predictor of development of a CTD than a positive ANA6,7. The distinction between PRP and SRP is important in view of the prognostic differences between the 2 groups. Patients with PRP tend to follow a mild clinical course, in contrast to the situation in patients with SRP, who may develop severe symptoms accompanied by digital ischemia8.
The difference in the prevalence of thumb involvement between PRP and SRP could also point to different pathophysiologies in PRP and SRP. The reasons for these differences were not addressed in this study. Our observations might mean that the thumb is less susceptible to reversible vasospasm that is a characteristic feature of PRP. An obliterative vasculopathy, one of the features of SSc, may be an important contributory factor in thumb involvement in SRP related to CTD.
Symptoms reported by patients could not be included in this retrospective study. However, in our previous prospective study we demonstrated reliability in symptom-reporting using thermography2.
Vasoactive drugs can potentially influence thermographic findings; for example, nifedipine has been shown to protect against a reduction in blood flow following a cold challenge in patients with RP9. Several of our patients were receiving vasodilator therapy; thus it is possible that this might have led to underestimation of patients with clinically relevant DDD in temperature, particularly in the SRP group, 48% of whom were on vasodilator therapy. Whether vasodilator therapy might have preferential effects on different digits is not known, but seems unlikely.
Thumb involvement may be of prognostic significance regarding the possibility of an underlying connective tissue disease or disorder; prospective studies are required to address these questions.
Footnotes
- Accepted for publication November 30, 2009.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.