

Abstract
Objective. To evaluate the association between the degree of involvement shown by parotid scintigraphy at diagnosis and the disease expression, outcomes, and prognosis of primary Sjögren’s syndrome (SS).
Methods. All patients consecutively diagnosed with primary SS in our department between 1984 and 2008 were evaluated. The scintigraphic stages were classified into class 4 (severe involvement), class 2–3 (mild to moderate involvement), and class 1 (normal results).
Results. A total of 405 patients with primary SS underwent parotid scintigraphy at diagnosis (47 had class 1 involvement, 314 had class 2–3, and 44 had class 4). Patients with class 4 had a higher frequency of parotid enlargement (p < 0.001), systemic involvement (p = 0.007), high titers of antinuclear antibody (p = 0.016), positive rheumatoid factor (p = 0.002), anti-Ro/SSA (p = 0.001), anti-La/SSB (p = 0.001), low C4 levels (p = 0.001), and low CH50 (p = 0.001) in comparison with the other 2 groups. A higher rate of lymphoma development was observed in patients with class 4 involvement. Adjusted multivariate Cox regression analysis showed a hazard ratio (HR) of 10.51 (p = 0.002) and Kaplan–Meier analysis a log-rank of 0.0005. Mortality was 5-fold higher in patients with class 4 involvement. Adjusted multivariate Cox regression analysis showed an HR of 5.33 (p = 0.001) and Kaplan-Meier analysis a log-rank of 0.033.
Conclusion. Patients with SS presenting with severe scintigraphic involvement at diagnosis had a more pronounced autoimmune expression, a higher risk of developing systemic features and lymphoma, and a lower survival rate. Study of the degree of salivary gland dysfunction at diagnosis by parotid scintigraphy offers valuable clinical information on the prognosis and outcome of primary SS.
Sjögren’s syndrome (SS) is a systemic autoimmune disease that presents with sicca symptomatology of the main mucosa surfaces1. The histological hallmark is a focal lymphocytic infiltration of the exocrine glands, determined by a biopsy of the minor labial salivary glands2. The spectrum of the disease extends from sicca syndrome to systemic involvement3,4. When sicca symptoms appear in a previously healthy person, the syndrome is classified as primary SS. When sicca features are found in association with another systemic autoimmune disease, most commonly rheumatoid arthritis, systemic sclerosis, or systemic lupus erythematosus, it is classified as associated SS.
As in other systemic autoimmune diseases, the diagnosis of SS is based on the fulfillment of a specific set of classification criteria, with the 1993 European criteria5 being the most frequently used and the 2002 American-European6 criteria the most recently proposed. In both sets of criteria, parotid scintigraphy is included as 1 of the 3 tests accepted for evaluating salivary gland dysfunction, with positivity being defined as delayed uptake, reduced concentration, and/or delayed secretion of the tracer, according to the method proposed by Schall, et al7. Several reports have studied the role of parotid scintigraphy in differentiating between SS and other causes of sicca syndrome8–10. However, no study has evaluated the clinical significance of the degree of scintigraphic involvement at diagnosis in a large cohort of patients with primary SS.
We evaluated the association between the degree of involvement shown by parotid scintigraphy at diagnosis and the disease expression, outcomes, and prognosis of primary SS in a large cohort of patients.
MATERIALS AND METHODS
Study cohort and observation time
The study cohort included 507 patients fulfilling the 1993 criteria for primary SS consecutively evaluated in our unit between 1984 and 2008. All patients were considered to have well established primary SS defined as fulfillment of at least 4 of the six 1993 SS criteria (including positive autoantibodies as mandatory criteria), the exclusion of other processes that may cause sicca syndrome (infiltrative processes, infections, or neoplasia), and the absence of other systemic autoimmune diseases. Nearly 80% of patients were referred from primary care centers and regional hospitals (the remaining patients were referred by other specialists from our hospital). Our clinical protocol required 6-monthly followups for all patients and 3-month followups for those with systemic involvement11,12.
Extraglandular involvement in primary SS was evaluated according to the clinical guidelines of the Spanish Society of Internal Medicine (SEMI) for the management of primary SS11,12. The following manifestations at diagnosis or during followup were defined as systemic features of primary SS: arthritis, Raynaud’s phenomenon, interstitial lung disease, renal involvement (interstitial nephritis or glomerulonephritis), vasculitis, pancreatitis, peripheral neuropathy (axonal polyneuropathy, multiplex multineuritis, or neuronopathy), cranial neuropathy, and central nervous system involvement (demyelinating disease, myelitis, or meningitis). Other features evaluated were severe parotid enlargement, oral infections (candidiasis, bacterial parotiditis), general features (fever, arthralgias), and organ-specific autoimmune features (both clinical and immunological). The entire cohort was retrospectively evaluated to determine fulfillment of the 2002 classification criteria6.
All patients were consecutively included when fulfillment of the SS classification criteria was confirmed by our unit and thereafter followed up prospectively with regular visits at 6- to 12-month intervals. Clinical and laboratory data were collected according to the standard protocol of the SEMI guidelines11,12. The individual observation time for every patient was from the time of fulfillment of the SS classification criteria until the last hospital visit, transfer out, or death. The study design conformed to current Spanish ethical standards. Because of the anonymous design of the study, informed patient consent was not required.
Parotid scintigraphy
Parotid scintigraphy is included in the routine diagnostic evaluation of patients with SS in our center. However, the test was not performed at diagnosis in 102 patients, mainly because of lack of agreement, contraindications, or noncompliance. Patients were injected intravenously with 185 MBq technetium pertechnetate and images were obtained immediately after injection to follow the accumulation phase. The patient lay supine and the camera was positioned frontally. A dynamic study of 60 min with 60 s per frame was carried out. Salivary gland scintigraphic data were gathered with a gamma-camera fitted with a low-energy high-resolution parallel-hole collimator, using a matrix size of 128 × 12813. The scintigraphic stages were determined according to the criteria proposed by Schall, et al7 and were classified by our 2 senior specialists in nuclear medicine into 3 subgroups (classes 2 and 3 were combined for statistical purposes and also because some results are borderline between these 2 classes): (1) class 4 (severe involvement — patients showing no active concentration in the salivary glands); (2) class 2–3 (mild to moderate involvement, defined according to the SS criteria6 — patients with delayed uptake, reduced concentration, delayed secretion of tracer, and/or absence of excretion into the oral cavity); and (3) class 1 (normal — patients with normal results (uptake of isotope occurring immediately after injection and concentration increasing progressively, with mouth activity appearing at 8–10 min).
Statistical analysis
Categorical data were compared using the chi-square and Fisher’s exact tests. Comparisons between dichotomous variables and the scintigraphy class variable were made by chi-square comparison of a 2 × 3 table, including the calculation of the Pearson chi-square (which is specified as the p value in the tables), the likelihood-ratio chi-square, and Yates’ corrected chi-square (continuity correction). Continuous variables were analyzed with the Student t-test in large samples of similar variance and with the nonparametric Mann-Whitney U test for small samples, with results indicated as mean ± standard error of the mean (SEM). A 2-tailed value of p < 0.05 was taken to indicate statistical significance. The outcomes measured were development of B cell lymphoma (defined according to the 2001 WHO classification for tumors of hematopoietic and lymphoid tissues14) and death. Univariate Cox regression analysis was used to evaluate the crude effect of the parotid scintigraphy involvement at diagnosis on outcomes. Multivariate Cox regression analysis using a backward stepwise method allowed adjustment for age, sex, and length of followup. The hazard ratios (HR) and 95% CI in the adjusted regression analysis were calculated. Kaplan-Meier survival curves were compared using the log-rank and Breslow tests. The statistical analysis was performed with SPSS (SPSS, Chicago, IL, USA).
RESULTS
A total of 405 patients clinically diagnosed with primary SS during the study period underwent parotid scintigraphy at diagnosis. There were 377 (93%) women and 28 (7%) men, with a mean age at time of fulfillment of the SS classification criteria of 57.27 years (SEM 0.73) and a mean followup of 86.82 months (SEM 2.91). Forty-seven patients were classified as having class 1 involvement, 314 as class 2–3, and 44 as class 4 in the parotid scintigraphy.
Association with disease expression
Epidemiologically, patients with class 4 involvement at diagnosis were older (p = 0.027) in comparison with those with class 1 involvement. Clinically, no significant differences were found in the prevalence of xerostomia, xerophthalmia, and altered ocular tests. Patients with class 4 involvement had a higher frequency of parotid enlargement (43% vs 17% in class 2–3 and 8% in class 1; p < 0.001) and systemic involvement (68% vs 43% and 45%, respectively; p = 0.007), including a higher frequency of vasculitis (16% vs 6% vs 2%; p = 0.020), lung disease (23% vs 16% vs 4%; p = 0.041), renal involvement (11% vs 2% vs 0%; p < 0.001), and peripheral neuropathy (18% vs 7% vs 13%; p = 0.042) in comparison with the other 2 groups (Table 1). Fulfillment of the 2002 criteria was higher in patients with class 4 involvement (73% vs 57% in class 1 and 49% in class 2–3; p = 0.01).
Epidemiologic features, sicca features included in the 2002 criteria, general features, associated organ-specific diseases, and systemic involvement of patients with primary SS according to parotid scintigraphic involvement. Data are no. (%), unless otherwise indicated.
With respect to laboratory features, patients with class 4 involvement had a higher frequency of raised erythrocyte sedimentation rate levels (27% vs 23% vs 7%, respectively; p = 0.027), anemia (23% vs 10% vs 2%; p = 0.005), leukopenia (29% vs 15% vs 9%; p = 0.017), high titers of antinuclear antibody (ANA; 54% vs 32% vs 23%; p = 0.016), positive rheumatoid factor (RF; 64% vs 39% vs 29%; p = 0.002), anti-Ro/SSA (57% vs 32% vs 22%; p = 0.001), anti-La/SSB (50% vs 23% vs 11%; p = 0.001), low C4 levels (21% vs 6% vs 2%; p = 0.001), and low CH50 (28% vs 9% vs 4%; p = 0.001) in comparison with the other 2 groups (Table 2).
Laboratory and immunological abnormalities of patients with primary SS according to parotid scintigraphic involvement. Data are no. (%).
Followup
In 40 patients, a second parotid scintigraphy was carried out a mean of 62 months after the initial diagnostic scintigraphy (range 12–140 months). Worsening in the degree of scintigraphic involvement was observed in 13 patients (32%), stabilization in 11 (27%), and improvement in 16 (41%). Patients who worsened had a higher frequency of altered immunological markers such as high titers (> 320) of ANA (75% vs 17%; p = 0.001) and a statistical trend to a higher prevalence of anti-Ro/La antibodies (38% vs 22%; p > 0.05), monoclonal circulating immunoglobulins (44% vs 26%; p > 0.05), cryoglobulins (15% vs 4%; p > 0.05), and low C4 levels (23% vs 4%; p > 0.05) in comparison with patients with stabilization/improvement. No significant differences were found according to the criteria fulfilled (worsening in 30% of 1993 patients vs 37% of 2002 patients) or a positive salivary gland biopsy (worsening in 33% of positive patients vs 67% of negative patients). A higher risk of developing oral candidiasis (15% vs 4%) and B cell lymphoma (8% vs 0%) was found in patients with worsening parotid scintigraphy, although the differences were not statistically significant.
Outcomes
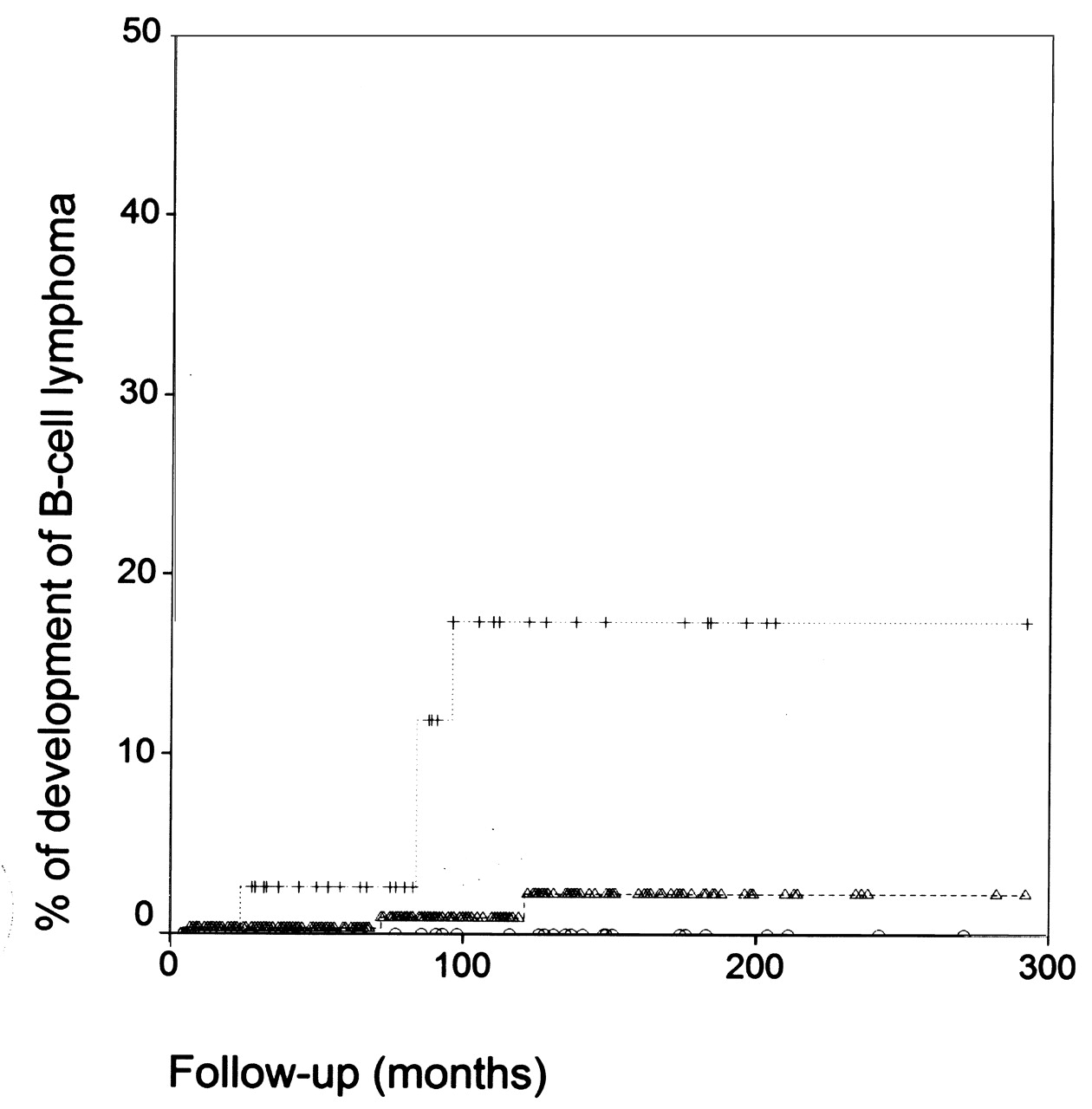
A higher rate of lymphoma development during followup was observed in patients with class 4 involvement in comparison with patients with a lower degree of involvement. Adjusted multivariate Cox regression analysis showed a HR of 10.51 (95% CI 2.35–47.00, p = 0.002) and Kaplan–Meier analysis showed a log-rank of 0.0005 (Figure 1).

Kaplan-Meier curves for the development of B-cell lymphoma according to the parotid scintigraphic involvement (crosses and broken line class 4, triangles and broken lines classes 2–3, bold line class 1, log rank = 0.0005)
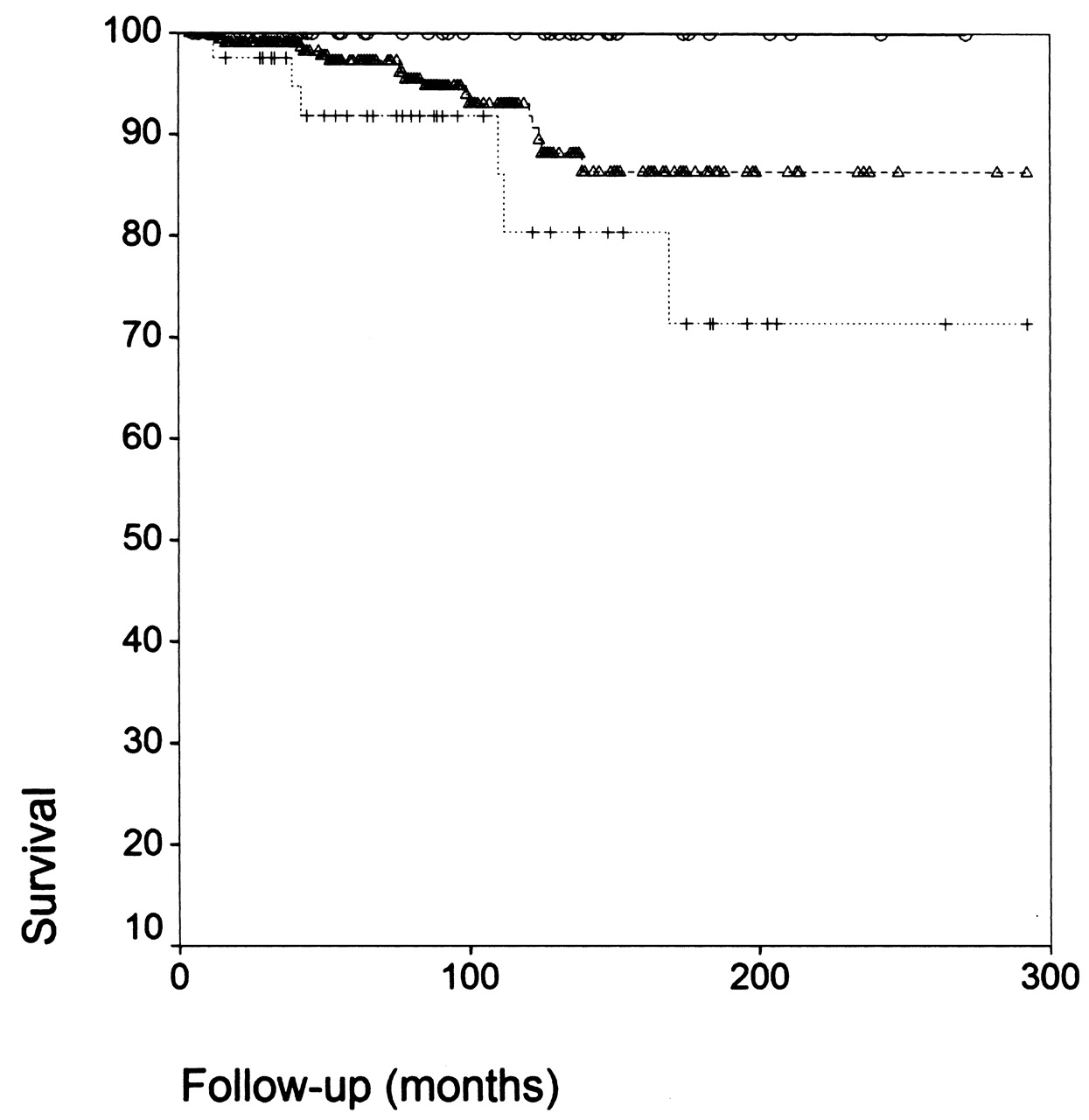
Mortality was 5-fold higher in patients with class 4 involvement. Adjusted multivariate Cox regression analysis showed a HR of 5.33 (95% CI 1.96–14.53, p = 0.001) and Kaplan-Meier analysis showed a log-rank of 0.033 (Figure 2).
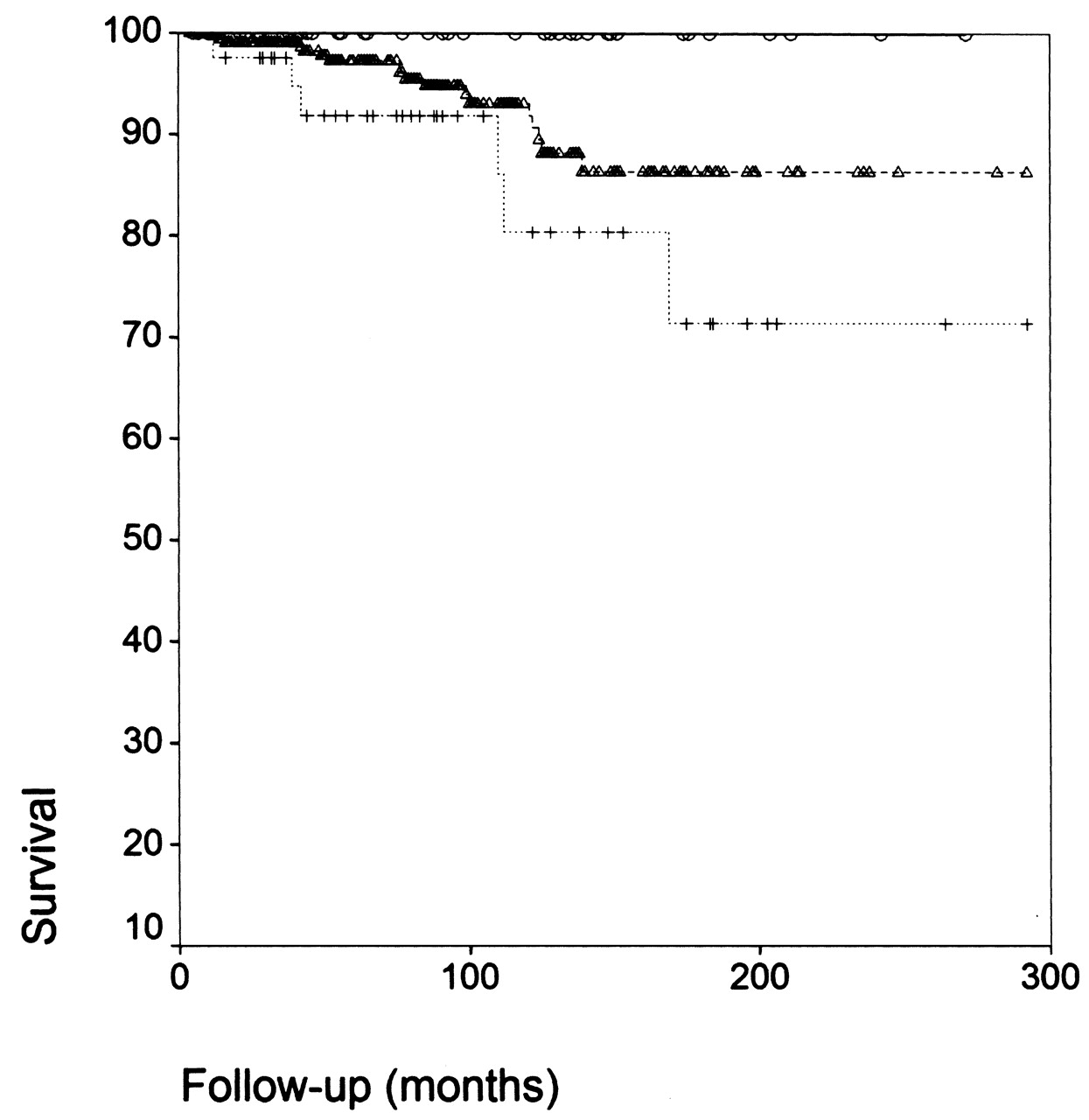
Kaplan-Meier survival curves according to the parotid scintigraphic involvement (crosses and broken line class 4, triangles and broken lines classes 2–3, bold line class 1, log rank = 0.033)
DISCUSSION
Salivary gland involvement in SS has traditionally been evaluated by sialography or minor salivary gland biopsy15–17. Although these tests have a high sensitivity and specificity, their diagnostic usefulness is limited by their invasive design16–19. In 1971, Schall, et al7 proposed a qualitative grade system for evaluating salivary gland function based on the results of quantitative analysis of (99mTc)-pertechnetate salivary gland scintigraphy, and subsequently, further grade systems were proposed20–22. However, Schall’s method was the one included in the 1993 classification criteria for primary SS7. In 2002, the American-European Consensus Group introduced some changes to the 1993 criteria in order to make the item definitions more precise and the tests more generally applicable. For salivary scintigraphy, a positive result was defined as delayed uptake, reduced concentration, and/or delayed secretion of the tracer, with no reference to any specific classification score. This has generated doubts about the correct application of this criterion, whose definition could correspond to classes 2 and 3 of Schall’s grade system7 but would not specifically include class 4, whose definition is “the complete absence of activity concentration of Tc-pertechnetate in major salivary glands”. In recent years, ultrasonography of major salivary glands has been introduced to study the parotid and submandibular glands of patients with SS. Ultrasonography is an inexpensive, noninvasive technique that is used to detect abnormalities in salivary glands23. Hypoechoic or anechoic areas are believed to represent lymphocytic infiltration and damaged salivary parenchyma, while cystic structures might reflect a progressive glandular destruction24. However, this technique still requires validation and comparison with the diagnostic tests included in the current criteria.
No studies have validated the clinical significance of the degree of parotid scintigraphy involvement in a large series of patients with primary SS. We found a significant correlation between parotid scintigraphy involvement and the disease expression and prognosis of primary SS. Patients diagnosed with class 4 involvement (the most severe degree of parotid involvement) had a higher risk of developing parotid enlargement and severe extraglandular features (vasculitis and renal, lung, and neurological involvement). A higher frequency of positive autoantibodies (Ro, La, and RF) and hypocomplementemia (an established immunological marker of adverse outcomes in primary SS25,26) and a higher risk of an adverse outcome (B cell lymphoma and death) were also found in patients with class 4 involvement in comparison with those with class 2–3 and, especially, with those with class 1. Patients with class 4 involvement had a 10-fold higher risk of developing B cell lymphoma and a 5-fold higher mortality rate compared with patients with less severe involvement at diagnosis. However, these findings should be confirmed in other cohorts of patients.
All previous studies were carried out in smaller series of patients with primary SS (usually, fewer than 80 cases) and focused overwhelmingly on the role of parotid scintigraphy in differentiating between SS and other causes of salivary gland dysfunction. These studies, using either qualitative or quantitative scintigraphic methods21,27–31, had a diagnostic sensitivity of 62%–89% and a specificity of nearly 50%. The low specificity of salivary gland scintigraphy is attributed to the fact that decreased uptake and delayed excretion of (99mTc)-pertechnetate is a nonspecific phenomenon common to all processes causing salivary gland dysfunction. Parotid scintigraphy reflects major salivary gland impairment and should be considered as nonpathognomonic for SS, because it is not useful in distinguishing, for example, between dysfunction due to autoimmune damage (lymphocytic infiltration) and that caused by external agents (radiotherapy). Therefore, the role of parotid scintigraphy in primary SS is to quantify the salivary gland dysfunction caused by the disease itself; it should not be used to differentiate between SS and other processes, a differential diagnosis that should be made clinically.
Few studies have investigated longterm salivary gland function in primary SS. Gannot, et al32 suggested that exocrine function, once compromised, remains stable over time, while Theander, et al33 described a rather stable course of the main manifestations of SS in a 5-year followup of 58 patients. Pijpe, et al34 have recently evaluated changes in salivary flow rate in 60 patients with SS (32 with primary SS) followed for a mean of 3.6 years, and found that although stimulated salivary flow rates decreased, there were no significant changes in baseline flow rates and sicca symptoms during the followup. This is the first study to focus on the results of a second parotid scintigraphy performed in 40 patients with primary SS after a mean of 5 years. The results confirmed the chronic, insidious course of salivary gland dysfunction, with more than two-thirds of patients showing stabilized or improved parotid scintigraphy. However, one-third of patients worsened after a mean of 7 years. Although the small number of cases did not allow statistically significant conclusions, patients who worsened had a more pronounced autoimmune expression and a trend to developing adverse outcomes. This suggests that parotid scintigraphy involvement may worsen in some patients with primary SS, which might result in poor outcomes. Although our study design did not let us conclude when and why the test should be repeated, we suggest that scintigraphy should be repeated every 2–3 years, at least during the first 10 years after diagnosis (the period with the worse prognosis26). In addition, repeat scintigraphy may be recommended in patients with significant worsening of oral symptoms and/or the development of oral complications such as severe caries, periodontal disease, or candidiasis.
Study of the degree of salivary gland dysfunction at diagnosis by parotid scintigraphy offers valuable clinical information on the prognosis and outcome of primary SS. Patients presenting with class 4 involvement at diagnosis had a more pronounced autoimmune expression, a higher risk of developing systemic features and lymphoma, and a lower survival rate, independently of the mean followup. Our results suggest that parotid scintigraphy involvement at diagnosis seems to clearly differentiate between patients with more aggressive disease (class 4 involvement), who have a poor outcome, and patients with a less pronounced systemic and immunological expression (class 1 involvement), who seem to have an excellent prognosis. This clearly suggests that parotid scintigraphy should be routine in all patients diagnosed with primary SS.
Acknowledgments
We thank David Buss for his editorial assistance.
Footnotes
-
Supported by Grants La Marató de TV3 (071810) and Fondo de Investigaciones Sanitarias (080103).
- Accepted for publication October 2, 2009.








{kind=link}
{kind=link}