

Vascular involvement is often present in dermatomyositis (DM). Severe nailfold capillaroscopy (NC) findings have been described but their association with disease activity and/or response to treatment have rarely been investigated1–7.
A 40-year-old man presented 6 months earlier for arthromyalgias, asthenia, fatigue, and muscle weakness, which was more evident at the lower limb level. He displayed erythematous-desquamative lesions on both hands, face, and neck, and Raynaud’s phenomenon.
Laboratory investigations showed erythrocyte sedimentation rate 54/h, C-reactive protein 48 mg/l, creatine kinase 530 U/l, lactate dehydrogenase 485 U/l, and anti-Jo-1 positivity. Electromyography examination of the upper and lower limbs revealed a myositic impairment with augmented junctional activity and presence of polyphasic potentials, while a muscle biopsy showed perivascular lymphomononuclear infiltrates with degenerative zones and necrosis.
The patient started 40 mg daily of 6-methylprednisolone (6-MP) but, owing to a progressive dyspnea, he was hospitalized. A pulmonary high-resolution computed tomography scan showed severe interstitial lung disease (ILD), more evident at periilar and basal levels, with a bilateral pleural effusion. Severely restrictive ventilatory impairment (forced vital capacity 55%; diffusion capacity for carbon monoxide 36%) and respiratory alkalosis were also present.
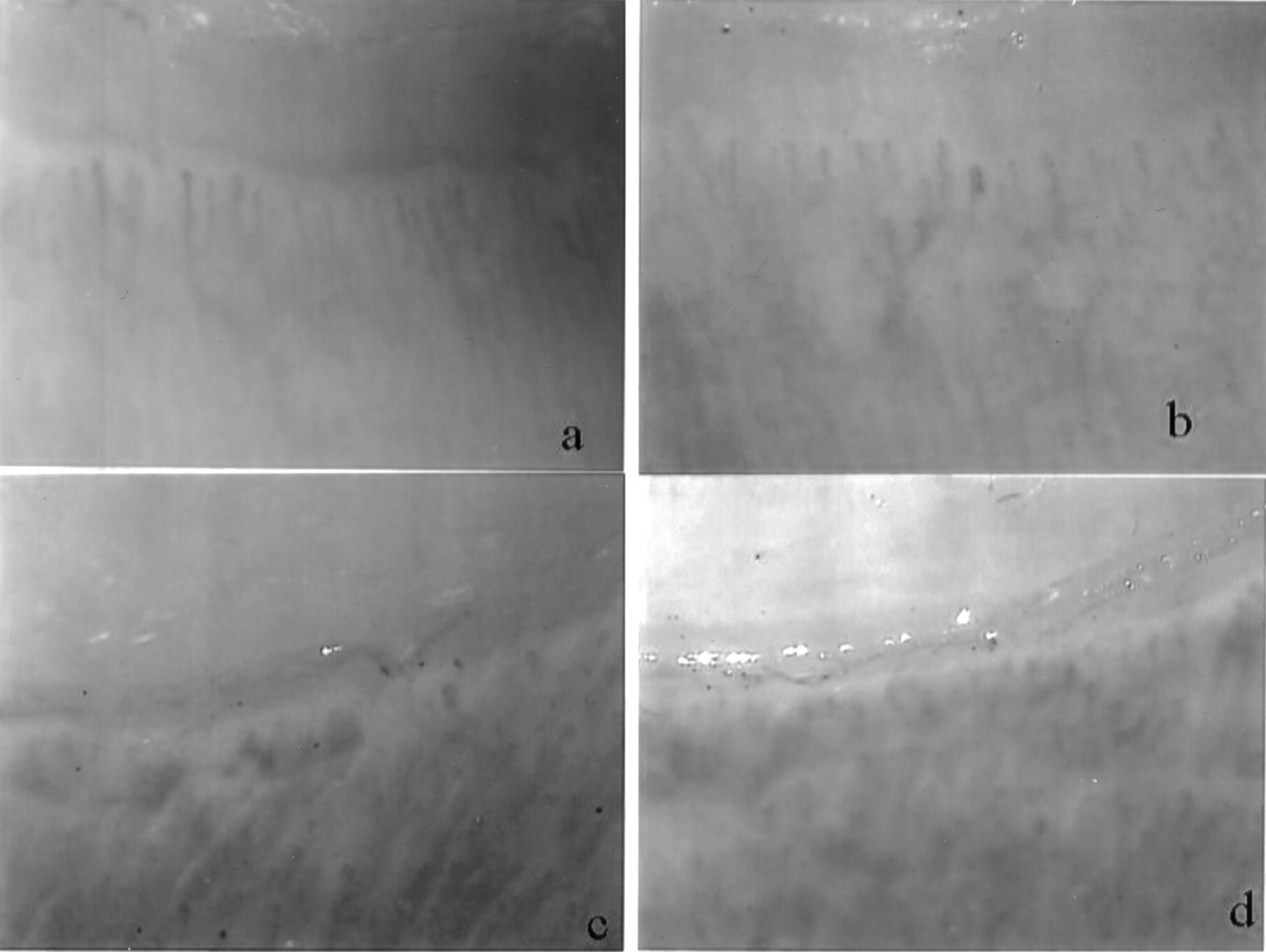
To evaluate Raynaud’s phenomenon we performed an NC, showing abnormal morphology, the distribution and number of the capillary loops with marked architectural derangement, frequent ramified and bizarre capillary loops, megacapillaries, and neoangiogenesis alternating with avascular areas. Frequent microhemorrhages were also found (Figure 1).

Nailfold capillaroscopy before immunosuppressive treatment, showing the index finger of the right hand (a), little finger, right hand (b), index finger, left hand (c), and ring finger, left hand (d). An abnormal morphology with irregular distribution and reduced number of capillary loops is shown, together with severe architectural derangement and presence of ramified and bizarre capillary loops in some fields. Megacapillaries, microhemorrhages, and neoangiogenetic features are also visible associated with some avascular areas.
A 6-month therapy with 750 mg/month cyclophosphamide (intravenous) was started, along with 80 mg/day 6-MP, gradually tapered to 8 mg/day. At the end of the treatment, the cutaneous lesions, strength, dyspnea, and muscle weakness improved. A mild basal interstitial involvement, with dyspnea on extended effort and restrictive lung impairment, was still present. Acute-phase reactants and serum muscle enzyme levels were within normal range. Table 1 shows the main clinical and laboratory changes during treatment.
. Main clinical and laboratory data of the patient at the start and after 6-month immunosuppressive treatment.
The NC was repeated on the same section of the nailfold, by the same observer, with the same magnification, and under the same environmental conditions. It revealed marked improvement, with normalization in the number, morphology, and distribution of capillary loops and neovascularized zones, and absence of microhemorrhages and giant capillaries (Figure 2). An immunosuppressive maintenance regimen was started with azathioprine 50 mg twice a day.
Nailfold capillaroscopy after 6 months of immunosuppressive treatment. (a) Index finger, right hand. (b) Little finger, right hand. (c) Index finger, left hand. (d) Ring finger, left hand. Marked improvement of capillaroscopic features is visible, with normal morphology, distribution and number of capillary loops, presence of revascularization, and absence of microhemorrhages and giant capillaries.
NC abnormalities are associated with skin involvement in untreated patients with DM3 and seem also to correlate with disease activity in inflammatory myopathies1,2. DM-specific NC changes in a scleroderma-like pattern8 provide useful information that contributes to an early diagnosis and helps identify those cases with a poor prognosis4. Owing to the possible fatal outcome of severe ILD in DM, an aggressive immunosuppressive regimen is recommended5,9.
Our case showed severe NC findings in a patient with DM and a clear improvement in these findings together with positive clinical and laboratory outcomes after immunosuppressive therapy, thus supporting the use of NC for diagnostic purposes and as a useful additional tool for followup and assessment of response to treatment in DM.








{kind=link}
{kind=link}