

To the Editor:
A 41-year-old woman with psoriatic arthritis developed watery diarrhea 3 days after starting diclofenac. She had been taking celecoxib for 3 years without having diarrhea. She also started taking etanercept 5 months prior to presentation. She stopped the diclofenac after 2 weeks of diarrhea, and her bowel movements returned to normal. She restarted the diclofenac 1 week later because of worsening joint pain, and her diarrhea recurred after 2 days. Her symptoms persisted despite permanently discontinuing the diclofenac 3 weeks later.
Four months after the onset of symptoms, she required admission to a hospital for dehydration. The etanercept was stopped. Her laboratory investigations, including complete blood count, electrolytes, erythrocyte sedimentation rate, albumin, kidney and liver function tests, tissue transglutaminase IgA antibody screen, and stool cultures, were all normal. A computed tomography scan of the abdomen was nondiagnostic. A colonoscopy revealed only mild erythema at the rectosigmoid junction. The pathologic examination of the biopsy specimen revealed marked thickening of the subepithelial collagen layer, and markedly increased numbers of inflammatory cells within the surface epithelium, consistent with severe collagenous colitis (Figure 1).
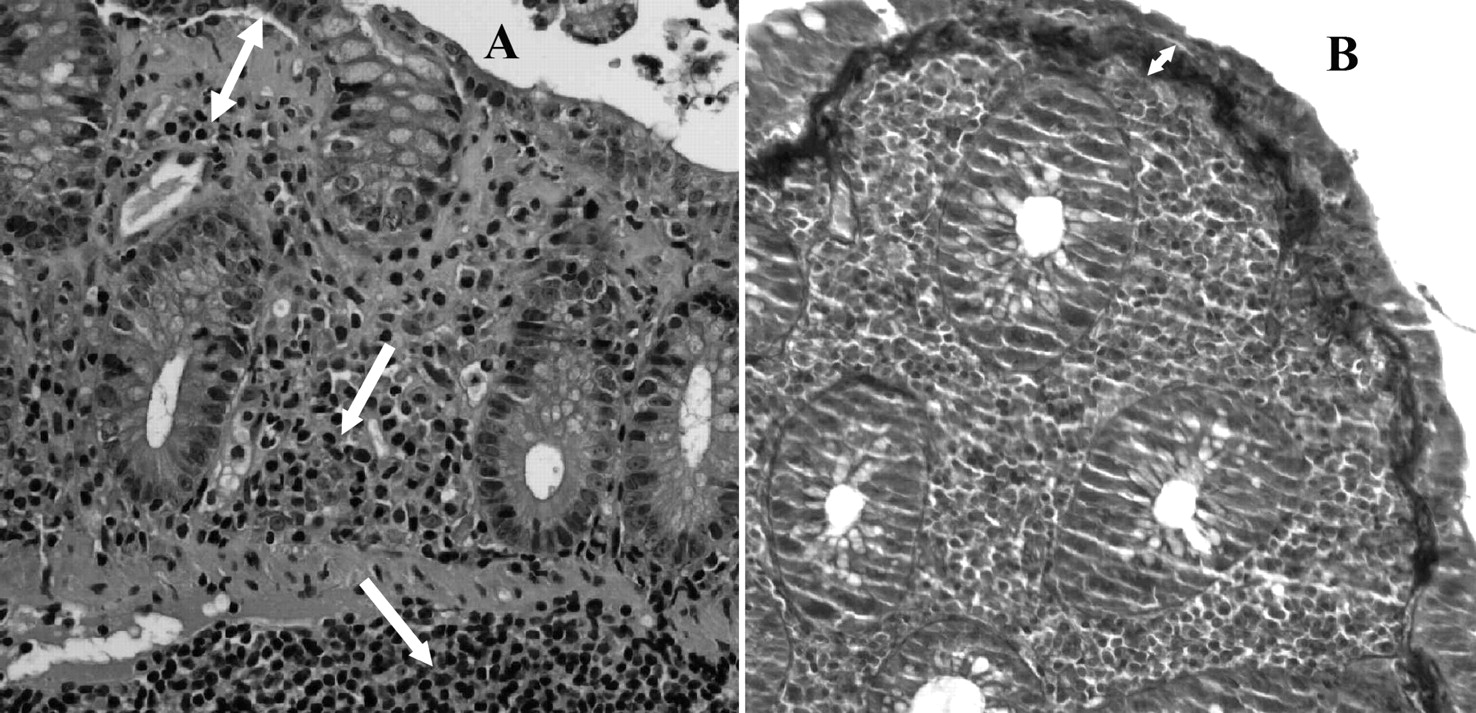
Patient’s biopsy samples. A: Hematoxylin and eosin stain, medium power. B: Mass on trichrome stain, medium power. White double arrows: collagen layer; white single arrows: inflammatory cells.
She was treated with oral budesonide, and her bowel movements returned to normal after 1 week of therapy.
Collagenous colitis (CC) is a diarrheal illness most commonly affecting patients in their fifth or sixth decade, with a distinct female predominance (3:1 to 8:1)1. Classically, patients present with chronic or intermittent watery diarrhea with or without abdominal pain, and usually without systemic symptoms1. Laboratory findings and imaging studies are often unremarkable, and the findings on colonoscopy are frequently nonspecific. CC is characterized pathologically by a thickened subepithelial collagenous band and intraepithelial infiltration with inflammatory cells. The annual incidence ranges between 1.1 and 5.2 per 100,0001. The cause of CC is not known. Between 20% and 60% of patients with CC have 1 or more autoimmune disorders, most commonly rheumatoid arthritis or thyroid disease1. CC is also associated with several drugs, most commonly nonsteroidal antiinflammatory drugs (NSAID), but also ticlopidine, proton pump inhibitors (PPI), antidepressants, and statins, among many others1. PPI are frequently used with NSAID for gastric protection, but our patient has never taken a PPI.
The precise incidence of CC among NSAID users is not known. The reported frequency of NSAID use in patients with CC ranges between 30% and 70%1. The mechanism of the association between NSAID use and CC is also not clear. It has been postulated that NSAID-induced inhibition of prostaglandin synthesis increases intestinal permeability and thus allows access of luminal contents to the lamina propria2. This causes inflammation and activation of the pericryptal fibroblasts, leading to thickening of the collagen layer2.
The length of NSAID use before the development of symptoms of CC ranges from weeks3 to over 15 years4, with the average being 5.5 years5. The duration of time to resolution of symptoms also varies, from days6 to several months2,7,8. In most patients, symptoms resolve spontaneously with discontinuation of the offending agent; some patients require additional treatment such as loperamide, budesonide, bismuth subsalicylate, sulfasalazine, 5-acetylsalicylic acid agents, or cholestyramine5,9.
Our case demonstrates a close temporal relationship between NSAID use and the development of CC. Several other papers describe the development of CC in the context of multiple challenges to NSAID. In a retrospective case-control study, Riddell, et al4 described a patient who developed symptoms twice after challenge with ibuprofen for the same length of time (6 months). Both times, diarrhea subsided immediately after stopping ibuprofen. In the same study, among the 8 cases for which precise temporal relationship between NSAID use and symptoms was described, diarrhea stopped in all 3 patients who stopped their NSAID, while symptoms continued in the remaining 5 patients who continued NSAID use. A case described by Al-Ghamdi, et al3 involved a patient who developed biopsy-proven CC initially after 6 weeks of taking diclofenac for osteoarthritis, and then again, 2 years later, after a 4-week course of ketoprofen. Both times, the patient’s symptoms resolved 2 weeks following discontinuation of the NSAID. In addition, this patient had a repeat colonoscopy and a normal biopsy 2 years after resolution of symptoms.
Of interest, our patient had been taking celecoxib, a selective cyclooxygenase-2 (COX-2) inhibitor, for 3 years before presentation. Her diarrhea, however, developed several days after switching to diclofenac, a nonselective COX inhibitor. Although it is possible that the longterm use of celecoxib contributed to the development of CC, the fact that the symptoms stopped after termination of diclofenac and then started again with rechallenge point to diclofenac as the more likely causative agent. Only a few cases of CC following the use of a selective COX-2 inhibitor have been described; we have identified 2 cases with rofecoxib1,2 and 2 cases with celecoxib1. This observation can be explained in part by the novelty of COX-2 inhibitors compared to the nonselective NSAID. However, there exists the possibility of a relative protective role of COX-2 selectivity in development of CC, similar to the effect on the upper intestinal tract. This remains to be investigated.
CC is rare, while NSAID use is extremely common. However, CC is a serious condition that is easily reversible if identified early. Therefore, physicians regularly prescribing NSAID need to keep CC in the differential diagnosis when evaluating a patient taking NSAID who presents with unexplained chronic watery diarrhea.
Acknowledgment
The authors thank Dr. Celia Marginean, Anatomic and Clinical Pathology, Ottawa Hospital.








{kind=link}