

Abstract
Objective. Mixed cryoglobulinemia (MC) is a systemic vasculitis of small and medium-size vessels, often associated with the hepatitis C virus. Research has shown an emerging role for chemokines and type 1 cytokines in the pathophysiology of this vasculitis. Interleukin 1 (IL-1) plays a role in initiating the cascade of immunoinflammatory responses, and levels of the interferon-γ (IFN-γ) inducible chemokine CXCL10 have been shown to be significantly associated with the presence of active vasculitis in patients with MC. We evaluated serum levels of IL-1ß, IFN-γ, and CXCL10 in a series of patients with hepatitis C-related MC (MC+HCV), and correlated these measurements with clinical disease features.
Methods. Serum IL-1ß, IFN-γ, and CXCL10 were assayed in 54 patients with MC+HCV, in 54 sex- and age-matched patients with type C chronic hepatitis without cryoglobulinemia (HCV+), and in 54 controls.
Results. MC+HCV patients showed significantly higher mean IL-1ß and CXCL10 serum levels than controls (p < 0.01) or HCV+ patients (p < 0.01). CXCL10 was significantly increased in 14 cryoglobulinemic patients with active vasculitis (necrotizing vasculitis or vasculitic skin ulcers) compared to those without (p < 0.001); IL-1ß was increased in cryoglobulinemic patients with active vasculitis (p = 0.06). No differences were observed for serum IFN-γ levels.
Conclusion. Serum levels of IL-1ß and CXCL10 were high in patients with MC+HCV. Increased CXCL10 and IL-1ß levels were associated with the presence of active vasculitis in MC+HCV patients.
Mixed cryoglobulinemia (MC) is a systemic vasculitis of small and medium-size vessels, associated with hepatitis C virus (HCV) in more than 90% of cases in an Italian series. Researchers have shown an emerging role for chemokines and Th-1 cytokines in the pathophysiology of this vasculitis. Involvement of the immune system in the pathogenesis of HCV-related MC (MC+HCV) has been reported1,2. Cytokines might be relevant in this context because of their central role in the immune response to viral agents3,4. Regarding Th-1 cytokines, serum concentrations of interferon-γ (IFN-γ) seem not to be significantly increased in patients with HCV or MC+HCV5,6; on the contrary, patients with HCV had high serum levels of tumor necrosis factor-α (TNF-α)7–9. Further, we have observed markedly high serum levels of IFN-γ inducible chemokine (CXCL10) and TNF-α in patients with MC+HCV compared to HCV patients and healthy controls; moreover, in patients with MC+HCV, increased CXCL10 levels were significantly associated with the presence of active vasculitis10.
Interleukin 1 (IL-1) includes 2 distinct proteins, IL-1α and IL-1ß, that play a central role in acute and chronic inflammation, both locally and systemically; it has an important role in initiating the cascade of immunoinflammatory responses through costimulation of T lymphocytes, B cell proliferation, induction of adhesion molecules, and stimulation of the production of other inflammatory cytokines11. IL-1 is produced primarily by monocytes and macrophages but also by astrocytes, adrenal cortical cells, natural killer (NK) cells, endothelial cells, T cells, and fibroblasts12. With IL-12, IL-1ß induces IFN-γ secretion by NK cells, resulting in an activation of macrophages that are IFN-γ induced11,12.
To our knowledge, few studies have evaluated the importance of IL-1ß in patients with MC13–16; no study has evaluated serum levels of IL-1ß in a large series of patients with MC+HCV in relation to the clinical phenotype.
One study showed that immune complexes containing either IgM/IgG or IgA/IgG aggregates from patients with type II essential MC induce IL-1 production in human peripheral blood monocyte-enriched populations13. Increased levels of IL-1ß were observed in patients with type C chronic hepatitis without cryoglobulinemia (HCV+) affected by non-Hodgkin’s lymphoma (NHL), but not in MC+HCV patients14. Further, IL-1ß was shown to be upregulated in pathologic tissue of patients with MC+HCV-related neuropathy and necrotizing arteritis15,16.
The aim of our study was to evaluate serum levels of IL-1ß, IFN-γ, and CXCL10 in a series of patients with MC+HCV, and to correlate these measurements with the clinical features of the disease.
MATERIALS AND METHODS
In patients and controls, a careful medical history was collected, in particular with regard to history of thyroid disease, smoking habits, and drugs. The presence of Raynaud’s phenomenon, Sjögren’s syndrome, skin ulcers, peripheral neuropathy, and renal and liver involvement in MC+HCV patients was evaluated17. Blood chemistry was investigated by standard methods18–20.
Thyroid screening was performed in all patients (history, physical examination, thyrotropin, free triiodo-thyronine, free thyroxine, antithyroglobulin and antithyroid peroxidase antibodies, ultrasonography) to exclude a thyroid autoimmune disorder, a well known cause of high serum CXCL1018–20. Patients with liver cirrhosis or hepatocellular carcinoma (by histology, laboratory evidence of liver failure, and/or ultrasound-proven portal hypertension)21,22 and thyroid autoimmune disorders were excluded. When a liver biopsy was performed, liver histology activity index (grade) and stage of liver fibrosis were evaluated according to Ishak, et al23.
The study protocol was approved by the local ethics committee. All subjects gave their informed consent to enter the study.
MC+HCV group
Fifty-four MC+HCV patients [39 women and 15 men; mean age 61 ± 12 (SD) years; mean disease duration 13 ± 9 (SD) years], consecutively referred to our Rheumatology Unit, were recruited for the study between 1999 and 2005. At the time of diagnosis, all patients showed clinico-serologic and pathologic features sufficient for a diagnosis of definite MC according to preliminary classification criteria1,2,17,24. Main demographic and clinico-serological features of MC+HCV patients are reported in Table 1.
Demographic and clinico-serological features of 54 patients with MC + HCV.
A total of 39/54 (72%) MC+HCV patients underwent liver biopsy; the mean activity index (grade) was 5.1 ± 1.2, and the stage was 2.0 ± 0.7. Among them, 19 had been previously treated with interferon-α (IFN-α) for an average of 7 months (range 1 to 15 mo), at a mean dosage of 10.1 MU/week; the time elapsed from the last course of IFN-α treatment ranged from 6 to 76 months (mean 42 ± 18 mo).
No statistically significant differences were observed in the main demographic and clinico-serological features of MC+HCV patients treated or untreated with IFN-α.
At the time of study, 40 MC+HCV patients were taking low doses of corticosteroids, while 8 had previously been treated with them. No MC+HCV patient had had plasma exchange treatment in the last year before the study.
Controls
Each of the 54 patients with MC+HCV eligible for the study were matched, by sex and age, 1 to 1 with a control group of healthy subjects of the general population from the same geographic area (northwest Tuscany). This control group was extracted from a larger sample of 1640 subjects in a population-based survey of thyroid disorders; only HCV-negative subjects, without clinical and laboratory evidence of thyroid and liver disorders and autoimmune diseases and not treated with immunomodulators, were included.
Another control group (HCV+) consisted of 54 sex- and age-matched patients with chronic HCV hepatitis without cryoglobulinemic syndrome (without other liver infection), extracted from a larger cohort of 491 chronic hepatitis referrals. Extraction of the control group from the original populations was performed by finding the closest age match (± 2 years) to each case within either gender. When more than 1 age match was available per case, the choice was made at random. Among them, 38 (70%) subjects underwent liver biopsy; the mean hepatitis activity index (grade) was 5.0 ± 1.0, and the stage was 2.1 ± 0.7.
Immunological studies
Cryocrit was measured as the percentage of packed cryoglobulins after cold centrifugation of the serum; cryoglobulin composition was determined by including the presence in cryoprecipitate of monoclonal or polyclonal IgM-rheumatoid factor (i.e., MC type II or MC type III); hemolytic complement C3-C4 fractions were measured17; antinuclear, anti-smooth muscle, and antimitochondrial autoantibodies were evaluated according to standard methodologies17. Sera with a titer > 1:40 were considered positive. Antiextractable nuclear antigen antibodies, including anti-Scl-70, -Sm, -RNP, -SSA/SSB, -PCNA, -SL and -Jo1 specificities, were detected by counter-immunoelectrophoresis, according to Bunn, et al25.
Virological studies
Antibodies against HCV (anti-HCV) and HCV-RNA were determined on serum clotted and centrifuged at 37°C and stored at −70°C. Anti-HCV and HCV-RNA (polymerase chain reaction technique) in the serum were investigated as described26,27.
Cytokines, chemokines, and analytical assays
Serum IL-1ß levels were assayed by a quantitative sandwich immunoassay using a commercial kit (R&D Systems, Minneapolis, MN, USA), with a sensitivity of < 0.5 pg/ml. The intra- and interassay coefficients of variation were 2.8% and 4.1%. Serum IL-1ß was detectable in 65% of controls and in all patients with MC+HCV and HCV+.
Serum CXCL10 levels were assayed by a quantitative sandwich immunoassay using a commercial kit (R&D Systems), with a sensitivity ranging from 0.41 to 4.46 pg/ml. The intra- and interassay coefficients of variation were 3.0% and 6.9%. Serum CXCL10 was detectable in all controls, in patients with MC+HCV, and patients with HCV+.
Serum IFN-γ concentrations were measured using commercial kits (R&D Systems). The mean minimum detectable dose was 8 pg/ml for IFN-γ and the intra- and interassay coefficients of variation were 2.9% and 6.3%. IFN-γ was detectable in the serum of 11% of controls, 17% of patients with HCV+, and 19% of patients with MC+HCV.
Samples were assayed in duplicate. Quality control pools of low, normal, or high concentration for all parameters were included in each assay.
Alanine aminotransferase (ALT) was assayed by conventional methods22.
Data analysis
Values are given as mean ± SD for normally distributed variables or as median ± interquartile range for non-normally distributed variables (IL-1ß). Group values were compared by univariate ANOVA, for normally distributed variables; or by Kruskal-Wallis (3 groups) or Mann-Whitney U (2 groups) tests. Proportions were compared by the chi-squared test. Post-hoc comparisons on normally distributed variables were carried out using the Bonferroni-Dunn test. Univariate analysis was performed by simple regression. A multivariate logistic regression analysis considering age, gender, ALT, IFN-γ, TNF-α, and presence or absence of active vasculitis as independent variables and presence or absence of high levels of CXCL10 as a dependent variable was performed in patients with MC+HCV. A simple regression was performed between CXCL10 and IL-1ß [log(pg/ml)].
RESULTS
Patients with MC+HCV showed significantly higher mean IL-1ß serum levels (mean 19 ± 41 SD ng/l; median 3.8 ng/l, range 0.7–168) than controls (mean 0.8 ± 0.3 SD ng/l; median 0.7 ng/l, range 0.7–1.7; p = 0.01) and patients with HCV+ (mean 3.1 ± 7 SD ng/l; median 1.1 ng/l, range 0.7–17; p = 0.04; median and range, Mann-Whitney U test; Figure 1). Patients with HCV+ showed slightly but not significantly higher mean IL-1ß serum levels than controls (Mann-Whitney U test).

Patients with mixed cryoglobulinemia and HCV chronic hepatitis (MC+HCV) showed significantly higher serum levels (mean ± SD) of interleukin 1ß (IL-1ß) than controls (p = 0.01) or patients with HCV+ (p = 0.04; Mann-Whitney U test).
By defining high IL-1ß level as a value higher than the 95th percentile of the control group (> 0.9 pg/ml), 59% (32/54) of patients with MC+HCV, 6% (3/54) of the control subjects, and 26% (14/54) of patients with HCV+ had high IL-1ß levels (p < 0.001, MC+HCV vs controls; p < 0.01, MC+HCV vs HCV+; p = 0.01, HCV+ vs controls; chi-squared).
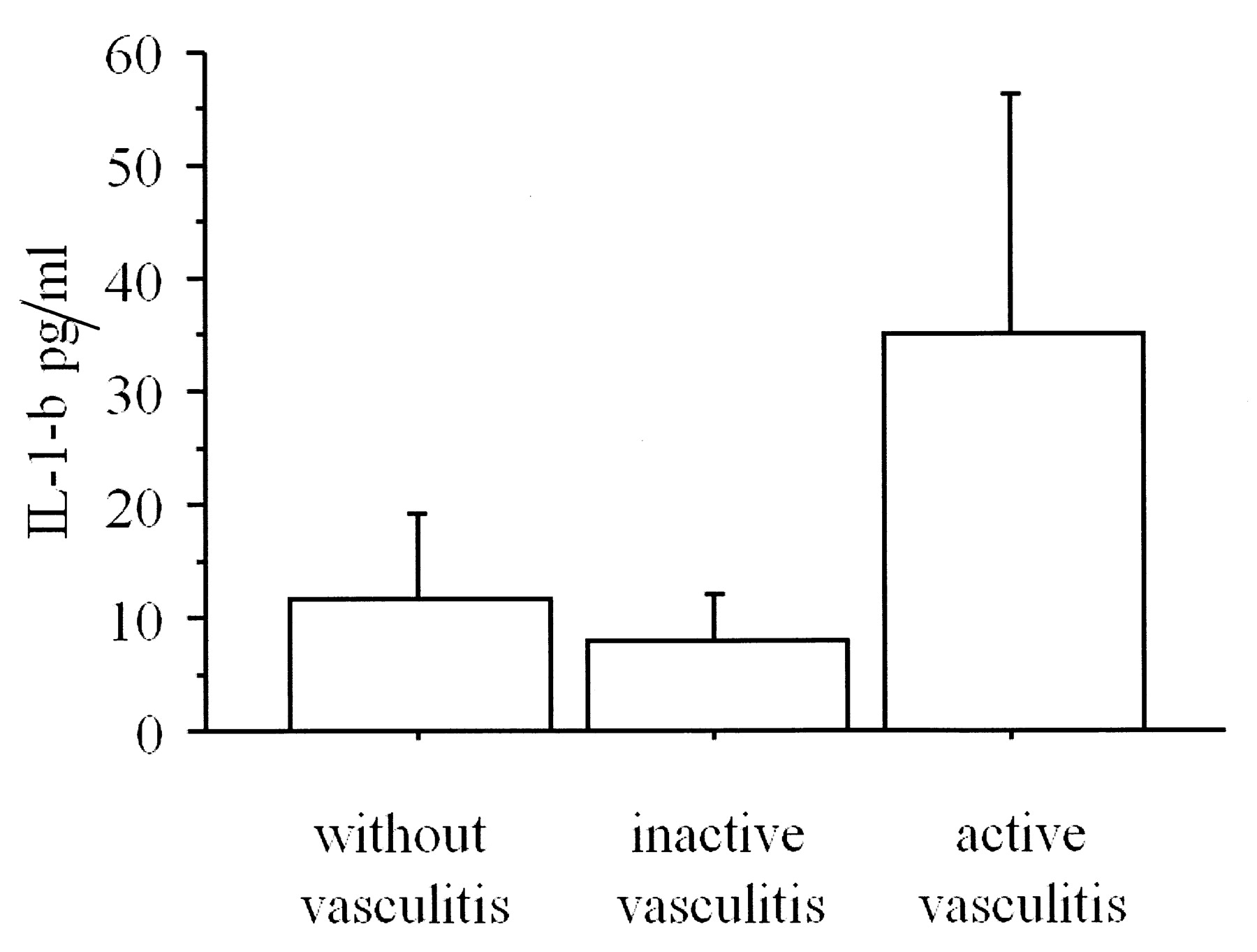
To better define the role of the increased serum IL-1ß in MC+HCV, mean levels of this chemokine were separately evaluated (by Mann-Whitney U test) among subgroups of patients with MC+HCV, defined according to main demographic and clinical features [age > 55 years, gender, disease duration > 10 years, presence or absence of purpura, active vasculitis (defined as necrotizing vasculitis with or without vasculitic skin ulcers), weakness, arthralgias, arthritis, Raynaud’s phenomenon, Sjögren’s syndrome, peripheral neuropathy, renal involvement, aminotransferase elevation, and/or histologic activity in the liver]. Higher levels of IL-1ß were observed in 14 patients with MC+HCV with active vasculitis at the time of the study in comparison to MC+HCV patients without signs of active vasculitis, or MC+HCV patients with inactive vasculitis (i.e., treatment-induced or spontaneous remission). However, statistical significance was not reached (Kruskal-Wallis, p = 0.06; Figure 2); no other significant result was found.
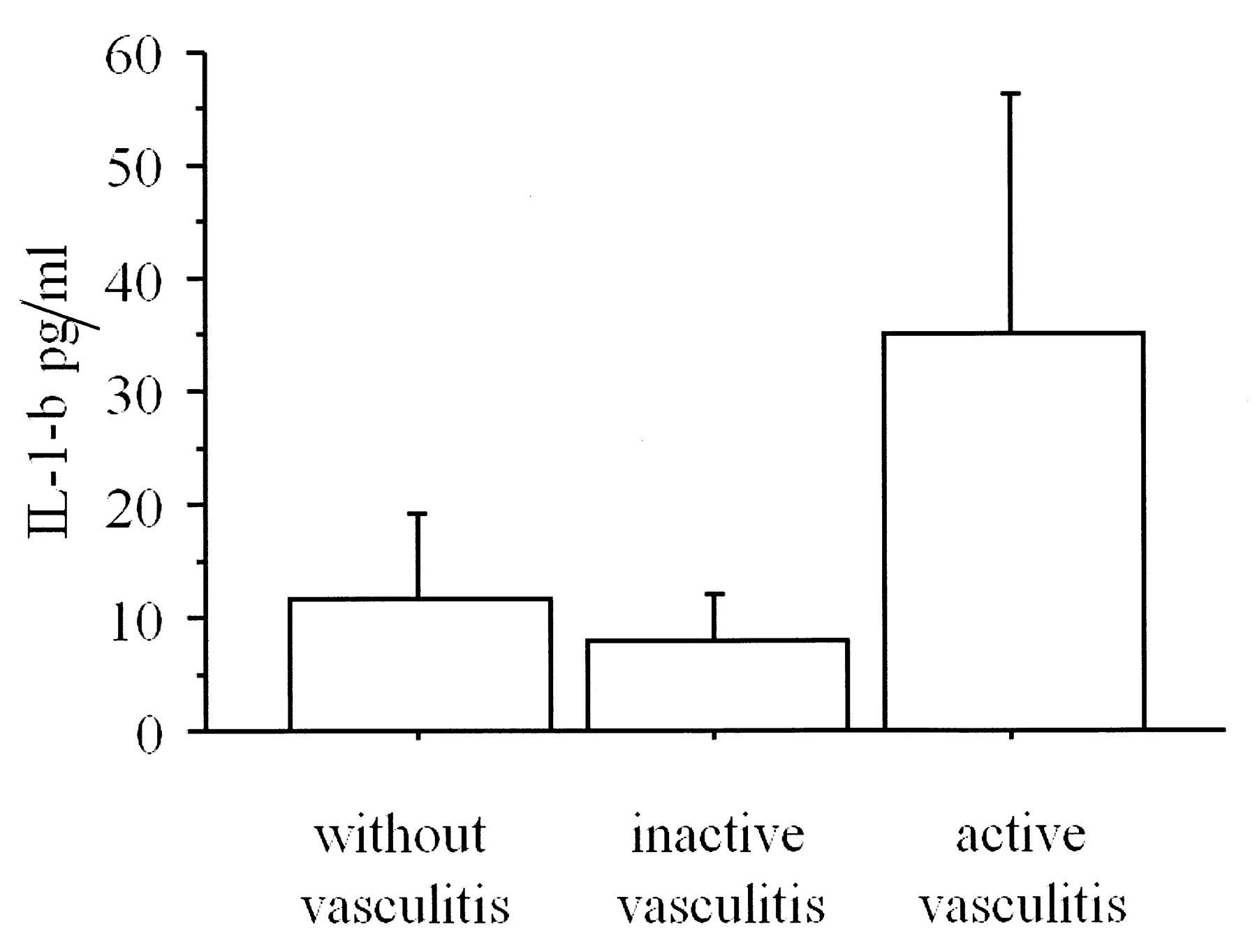
Higher serum levels of interleukin 1ß (IL-1ß; mean ± SD) were observed in patients with MC+HCV with active vasculitis at the time of the study in comparison to MC+HCV patients without signs of active vasculitis or MC+HCV patients with inactive vasculitis (i.e., treatment-induced or spontaneous remission). However, statistical significance was not achieved (Kruskal-Wallis p = 0.06).
No significant correlations were observed between IL-1ß and serological findings of MC+HCV (levels of cryocrit and complement, presence/absence of autoantibodies, type 2/type 3 cryoglobulins), or previous/ongoing treatments.
Patients with MC+HCV showed significantly higher mean CXCL10 serum levels than controls (p < 0.0001) or patients with HCV+ (p < 0.0001; 381 ± 127 pg/ml; 90 ± 51 pg/ml; 270 ± 151 pg/ml, respectively; ANOVA). Patients with HCV+ showed significantly higher mean CXCL10 serum levels than controls (p < 0.0001; ANOVA).
To better define the role of serum CXCL10 in patients with MC+HCV, mean levels of this chemokine were separately evaluated (by ANOVA) among MC+HCV patient subgroups defined according to main demographic and clinical features as above. Significantly higher levels of CXCL10 were observed in 14 patients with active vasculitis at the time of the study in comparison to those without (433 ± 112 vs 348 ± 127 pg/ml, respectively; p < 0.01); no other significant result was found. Both groups of MC+HCV patients with or without active vasculitis had serum CXCL10 significantly higher than patients with HCV+ (p < 0.01 and p = 0.03, respectively, ANOVA).
By defining high CXCL10 level as a value of at least 2 SD above the mean value of the control group (> 192 pg/ml), 78% of patients with MC+HCV, 4% of the control subjects, and 61% of patients with HCV+ had high CXCL10 levels (p < 0.0001, for both, MC+HCV vs controls or HCV+ vs controls; chi-squared).
No significant correlations were observed between CXCL10 and serological findings of MC+HCV (levels of cryocrit and complement, presence/absence of autoantibodies, type 2/type 3 cryoglobulins) or previous/ongoing treatments.
IFN-γ was detectable in the serum of 11% of controls, 17% of patients with HCV+, and 19% of patients with MC+HCV (chi-squared, p = nonsignificant); IFN-γ levels were not significantly different in the 3 groups.
Patients with HCV+ and patients with MC+HCV had, obviously, raised alanine aminotransferase (ALT) enzymes in comparison with controls (p < 0.0001); however, there was no significant difference in serum ALT between patients with HCV+ and patients with MC+HCV. No association was observed between IL-1ß or CXCL10 levels and ALT levels in either patients with HCV+ or patients with MC+HCV. No relationship was observed between CXCL10 and IL-1ß [log(pg/ml)] by a simple regression. The activity index (grade) and the stage in patients with HCV+ and in patients with MC+HCV were not significantly different. No association was observed between IL-1ß or CXCL10 concentration and liver histology activity index or stage of liver fibrosis in each group, or when considering the 2 groups together.
DISCUSSION
The role of the immune system and of Th1 and Th2 cytokines in the hepatic and extrahepatic manifestations of the HCV has been widely investigated. Their expression could be useful to differentiate HCV-related vasculitis from other systemic vasculitis5–8,14,15,28,29 (Table 2). Our study demonstrates significantly high serum levels of IL-1ß in patients with MC+HCV compared to healthy controls and patients with HCV+. Among patients with MC+HCV, the IL-1ß levels tended to be higher, even if not significantly, in patients with signs of active vasculitis compared to those without.
Cytokine concentrations in HCV-related disorders and systemic vasculitis.
Further, our study confirms significantly high serum levels of CXCL10 and TNF-α in patients with MC+HCV compared to healthy controls10. High levels of serum CXCL10 were found in patients with HCV chronic infection without cirrhosis, as previously reported30–33. Interestingly, the baseline level of CXCL10 (measured before the start of antiviral treatment) was greatest in patients with HCV who subsequently became nonresponders to the treatment31,34; among MC+HCV the CXCL10 levels were significantly higher in patients with signs of active vasculitis compared to those without.
IL-1ß is a cytokine belonging to the innate immune system that plays an important role in initiating the cascade of events of immunoinflammatory responses, by binding to specific high-affinity cell-surface receptor type II in synergy with the interleukin receptor accessory protein35. IL-1ß shows pleiotropic effects that include costimulation of T lymphocytes, B cell proliferation, growth of fibroblasts, induction of adhesion molecules, stimulation of production of other cytokines and inflammatory mediators, and growth-inhibitory and cytocidal effects for several cell lines36.
Our observation of high levels of circulating IL-1ß in MC+HCV is in agreement with 2 other studies. In the first, immune complexes containing either IgM/IgG or IgA/IgG aggregates were shown to induce IL-1 production in human peripheral blood monocyte-enriched populations from patients with type II essential MC13. In the second study, the quantitative expression levels of 42 selected genes involved in inflammatory vascular damage were assessed in nerve lesions of patients with MC+HCV vasculitis, polyarteritis nodosa, and noninflammatory idiopathic neuropathy, using real-time reverse transcriptase-polymerase chain reaction. The expression of IL-1ß was shown to be upregulated in pathologic tissue of patients with MC+HCV neuropathy and necrotizing arteritis15. This may be particularly relevant here, since 78% of our patients with MC+HCV have peripheral neuropathy.
Libra, et al evaluated circulating levels of IL-1ß in 14 patients with HCV+, in 20 patients with MC+HCV, and in other patients with HCV+ with NHL (in presence or absence of MC). An increase of circulating levels of IL-1ß was observed only in patients with HCV+ and concurrent NHL14.
Our observation of a higher value of IL-1ß in patients with MC+HCV with active vasculitis is compatible with an upregulation of IL-1ß expression in MC+HCV patients with necrotizing arteritis15.
The main site of IL-1ß production in MC+HCV subjects remains to be clarified: IL-1ß is normally produced by monocytes and macrophages12, so it is possible that these cell types may participate in elevating IL-1ß in MC+HCV, while it is unlikely that the liver is the site of cytokine production. The finding of higher levels of IL-1ß in patients with MC+HCV with active vasculitis seems to reinforce this hypothesis, even if a participation of endothelial cells cannot be excluded11,12. Further studies are needed to clarify the cellular source of IL-1ß in MC+HCV.
Our study confirms significantly high serum levels of CXCL10 in patients with MC+HCV compared to healthy controls, above all in patients with signs of active vasculitis; however, no relation was observed between IL-1ß and CXCL10 levels, suggesting that vasculitis in MC+HCV patients is associated with an independent increase of both cytokines10. Studies in larger series of patients will be needed to evaluate the relevance of serum CXCL10 determination as a marker of MC+HCV with active vasculitis. The increase of CXCL10 in both patients with HCV+ and patients with MC+HCV suggests that the liver may be an important site of secretion.
Interestingly, increased serum levels of another CXCR molecule, the chemokine CXCL13, and upregulation of its gene expression have been shown to be distinctive features of HCV-related cryoglobulinemia and to correlate with active cutaneous vasculitis37.
Harvey, et al tried to define the cellular source of CXCL10 in the liver by immunohistochemistry and to correlate CXCL10 expression with the histological markers of liver inflammation38. CXCL10 was expressed by hepatocytes, but not by other cell types within the liver. These findings suggest that CXCL10 may be induced by the HCV within hepatocytes and may be important in the pathogenesis of chronic HCV hepatopathy, since recruitment of inflammatory cells into the lobule is an important predictor of disease progression39. However, since CXCL10 is significantly increased in MC+HCV patients with active vasculitis more than in HCV+ patients with a similar degree of liver involvement, the liver inflammation and other autoimmune manifestations of MC may act synergistically in the elevation of serum CXCL10 levels in these patients10.
Change of serum chemokine levels in the course of other autoimmune disorders has been demonstrated. Recent experiments have shown that CXC chemokines, and particularly CXCL10, play an important physiopathological role in the initial phases of autoimmune thyroid disorders40–44, with an inverse correlation between circulating CXCL10 levels and disease duration in Graves’ disease (GD)40.
In our study we found no relation between serum IL-1ß levels and the duration of MC+HCV, probably because of the relapsing clinical course of the disease, in particular in vasculitic manifestations; these complications may appear at any time during the followup, possibly triggered by multiple pathogenetic cofactors2. Clinico-pathological alterations of MC+HCV may recognize at least 2 synergistic pathogenetic mechanisms triggered by HCV: B cell proliferation leads to immune complex production, mainly HCV-containing cryoglobulins16, which are responsible for immune complex-mediated vasculitis1,2,17,26; at the same time high serum IL-1ß levels strongly amplify the inflammatory process through costimulation of T lymphocytes and B cell proliferation.
The increase of IL-1ß and CXCL10 in the active phase of the disease is in agreement with previous reports of high serum CXCL10 values in the active phase of multiple sclerosis and GD. Indeed, CXCL10 is upregulated at disease onset and during relapse in multiple sclerosis45–47. Further, we have recently shown that increased serum CXCL10 levels in patients with GD are associated mainly with the active phase of GD19,48.
Longitudinal studies evaluating serum IL-1ß and CXCL10 levels in large series of patients with MC+HCV will be needed to evaluate whether serum IL-1ß and/or CXCL10 measurement could represent an easily detectable prognostic marker for clinical management of patients with MC+HCV.
Regarding Th1 cytokines, our study confirmed that serum levels of IFN-γ are not significantly increased in patients with HCV+ or patients with MC+HCV. This is in accord with other studies of patients with HCV5,6,10.
We observed significantly high serum levels of IL-1ß in patients with MC+HCV compared to healthy controls and patients with HCV+, above all in patients with signs of active vasculitis. Further, significantly high serum levels of CXCL10 in patients with MC+HCV compared to healthy controls are confirmed in the presence of active vasculitis. Future studies in larger series of patients will be needed to evaluate the relevance of serum IL-1ß and CXCL10 determination as clinico-prognostic markers of MC+HCV, as well as its usefulness in the therapeutic approach to these patients.
Footnotes
- Accepted for publication August 12, 2009.








{kind=link}
{kind=link}