

A 71-year-old woman with Sjögren’s syndrome and giant cell arteritis was treated with intravenous immunoglobulin (IVIG) (6 g protein/250 ml, stabilized with sucrose 10 g/flacon, NaCl 0.02 g/g protein) for peripheral sensory motor neuropathy — an unlabeled use of the drug1,2.
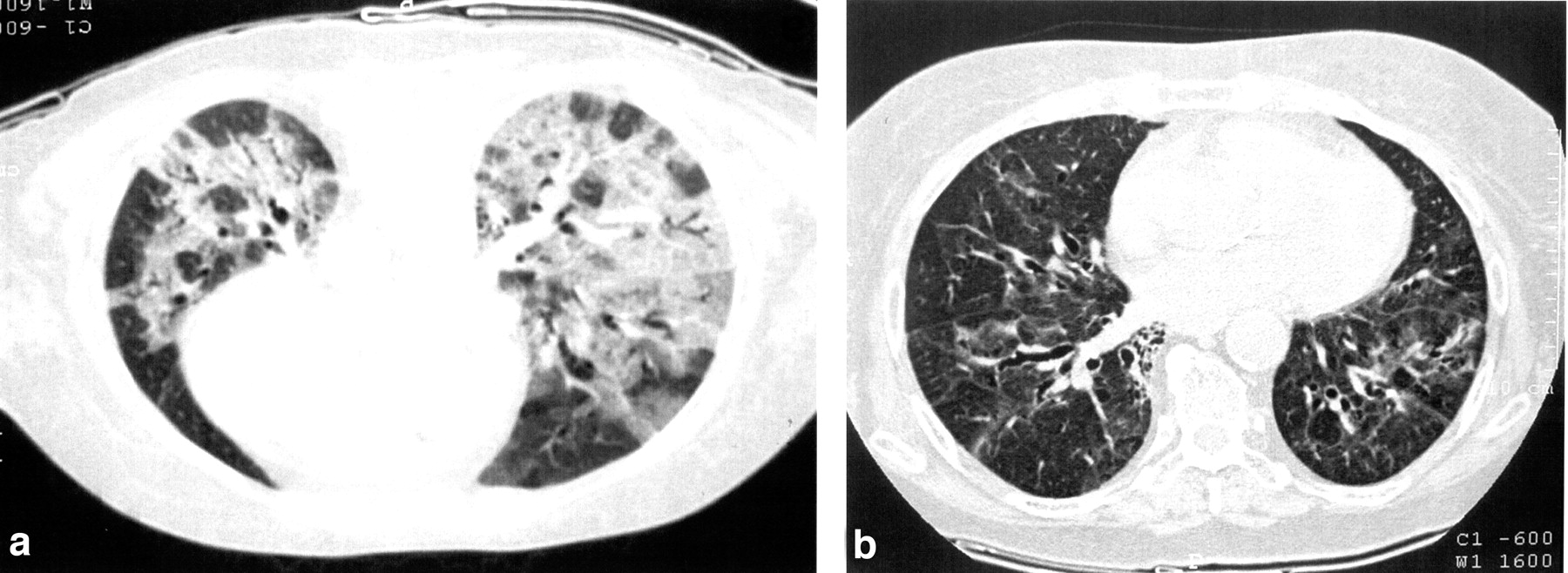
The dose of IVIG was 400 mg/kg/day for 5 days. During administration of the third flacon of IVIG (12 grams had been already infused over 4 hours with an infusion rate ~2.1 ml/min), the patient presented increasing dyspnea. Physical examination showed bilateral rales, a pulse of 95 beats per min and blood pressure of 130/70 mmHg, PO2 of 45.7 torr, and Sat O2 83.8%. A chest radiograph showed interstitial and airspace infiltrates. IVIG was discontinued. Computed tomography (CT) of the chest revealed alveolar infiltrates bilaterally (Figure 1). Transfusion-related acute lung injury (TRALI) was diagnosed based on acute respiratory distress, bilateral lung infiltrations in the radiograph (which occurred within 6 h of transfusion of IVIG), hypoxemia, Sat O2 < 90%, and no evidence of transfusion-associated cardiogenic lung edema, anaphylactic reaction, or sepsis. Other risk factors for acute lung injury (aspiration, pneumonia, toxic inhalation, lung contusion, shock) were excluded3. The patient was treated with a continuous positive airway pressure mask maintaining saturation above 90%. There was a gradual improvement of arterial blood gas and CT findings during the next 4 weeks (Figure 2).
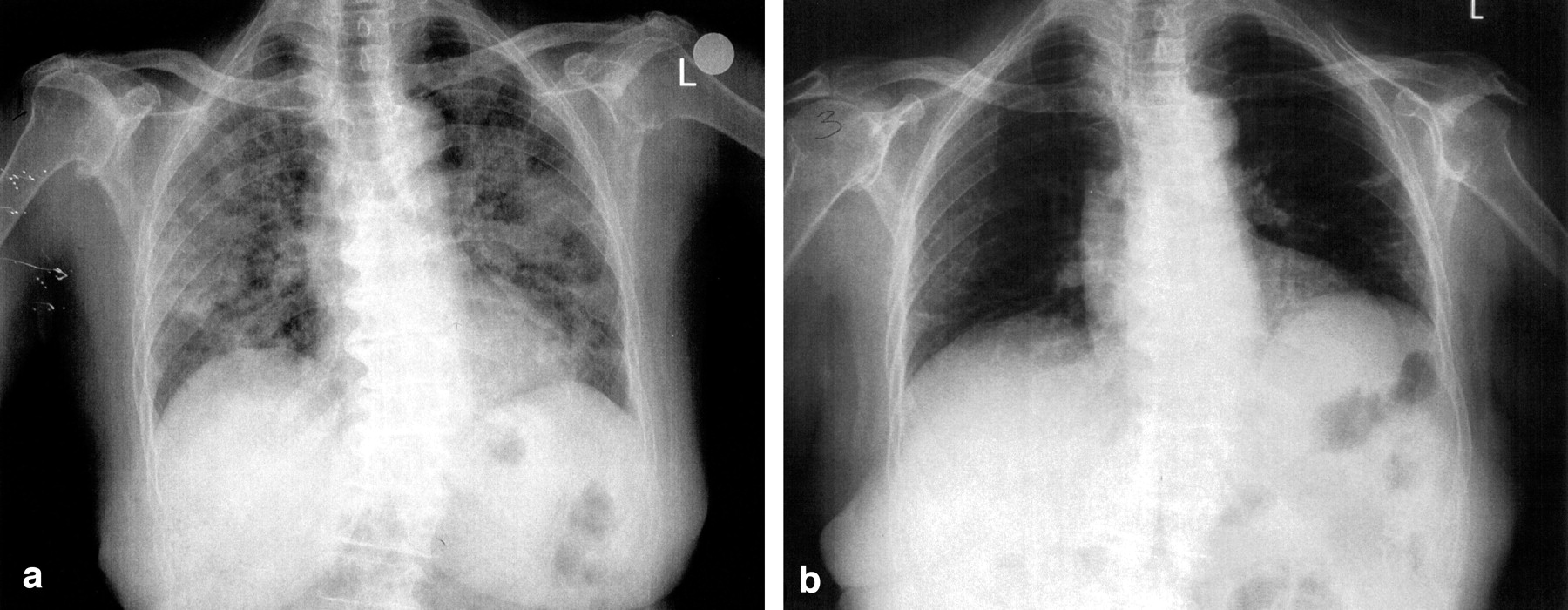
(A) Extensive coalescent airspace infiltrates bilaterally. (B) Great improvement of the radiological findings of the lungs.

(A) Computed tomography of the thorax: coalescent pulmonary infiltrates and areas with ground glass appearance. (B) Areas of ground glass appearance in the position of preexisting infiltrates. Existence of bronchiectasis in the same area.
Few cases of TRALI after IVIG have been described4. Leukocyte antibodies and neutrophil priming agents released in stored cellular blood components have been considered causative. The mainstay of therapy is oxygen and when needed, ventilatory support. The presence of neutrophil antibodies in the IVIG and cognate neutrophil antigens in the patient were not investigated. According to the published criteria5, although her clinical course was atypical, this case strongly suggests TRALI after IVIG.








{kind=link}
{kind=link}