

To the Editor:
A 19-year-old female college student presented to the emergency room with sudden onset of palpitations while watching a movie. Her history was unremarkable, and she denied any abuse of alcohol, recreational drugs, or over-the-counter stimulants. Review of systems was negative for any recent fever, rash, sick contacts, or acute illness involving the respiratory or gastrointestinal tract. Vital signs on presentation were notable for a temperature of 100.1°F, a regular tachycardia at 220 beats per minute, and blood pressure 120/70 mm Hg. The remainder of the examination and a chest radiograph were unremarkable. The electrocardiogram showed a wide complex tachycardia with monophasic right bundle branch morphology in lead V1 and right inferior QRS axis (Figure 1). Intravenous procainamide was administered, with prompt restoration of sinus rhythm. The sinus rhythm electrocardiogram was normal. Transthoracic echocardiography revealed normal left ventricular function, homogeneous enlargement of the anterolateral papillary muscle, and mild mitral regurgitation (Figure 2). Differential diagnosis included a cardiac tumor, unusual isolated papillary muscle hypertrophy, or an infiltrative systemic process, such as sarcoidosis or Wegener’s granulomatosis. Erythrocyte sedimentation rate was 56 mm/h with a white cell count of 11,900 k/μl. Initial urine examination revealed more than 50 red blood cells and 3–5 white blood cells per high power field and trace protein, with subsequent repeat urinalysis that was normal. Thoracoabdominal computed tomography showed no lymphadenopathy, metastatic disease, or other abnormalities.
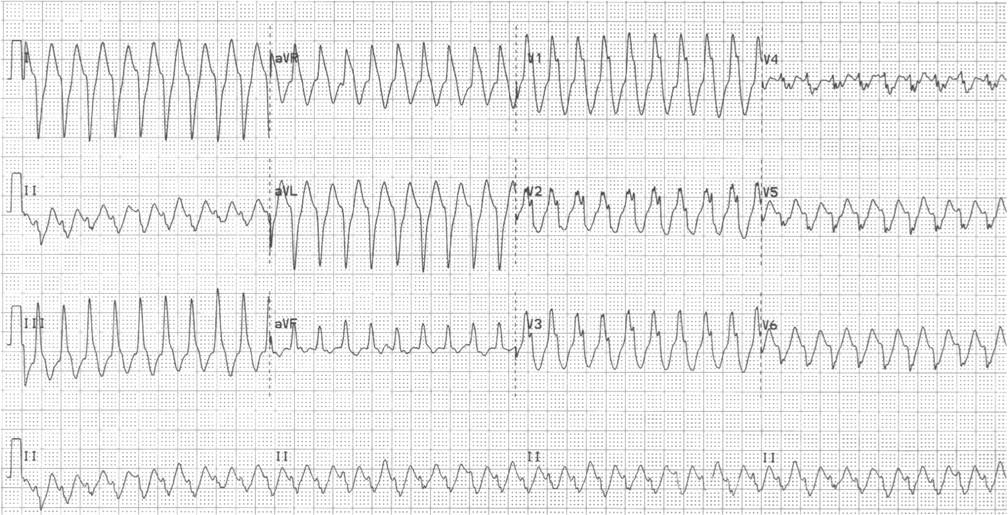
At presentation, electrocardiogram shows ventricular tachycardia.
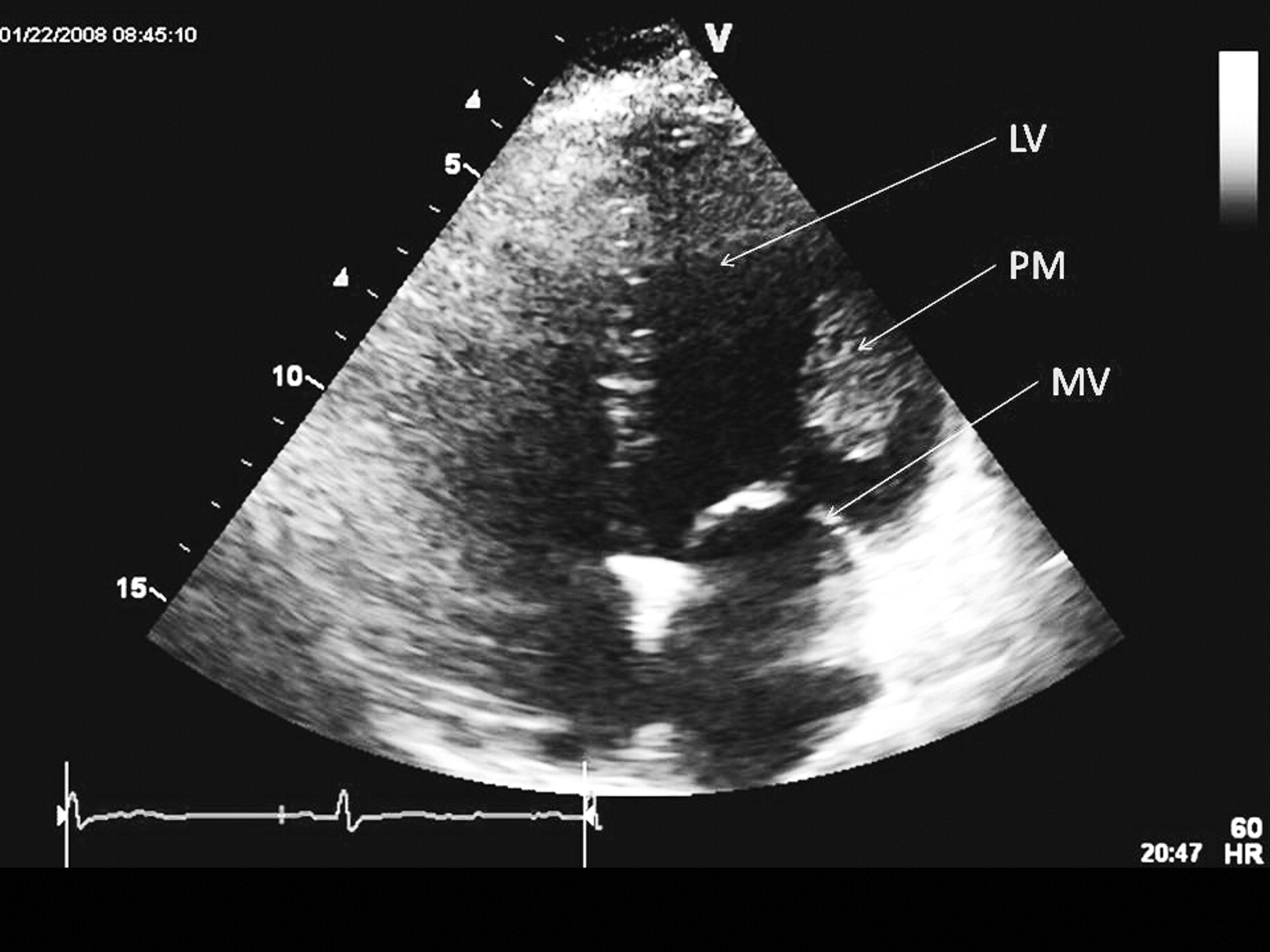
Transthoracic echocardiogram. PM: anterolateral papillary muscle mass; LV: left ventricle; MV: mitral valve.
Cardiac magnetic resonance imaging (MRI) was performed for further tissue characterization. Thickening of the anterolateral papillary muscle was seen on functional steady-state free precession images. On T1-weighted imaging the mass appeared isointense, and on T2-weighted imaging the mass was hyperintense. Following administration of intravenous gadolinium, the mass was seen to enhance, suggesting scarring or fibrosis (Figure 3). The lack of other endocardial involvement, including the adjacent anterolateral wall, was confirmed.
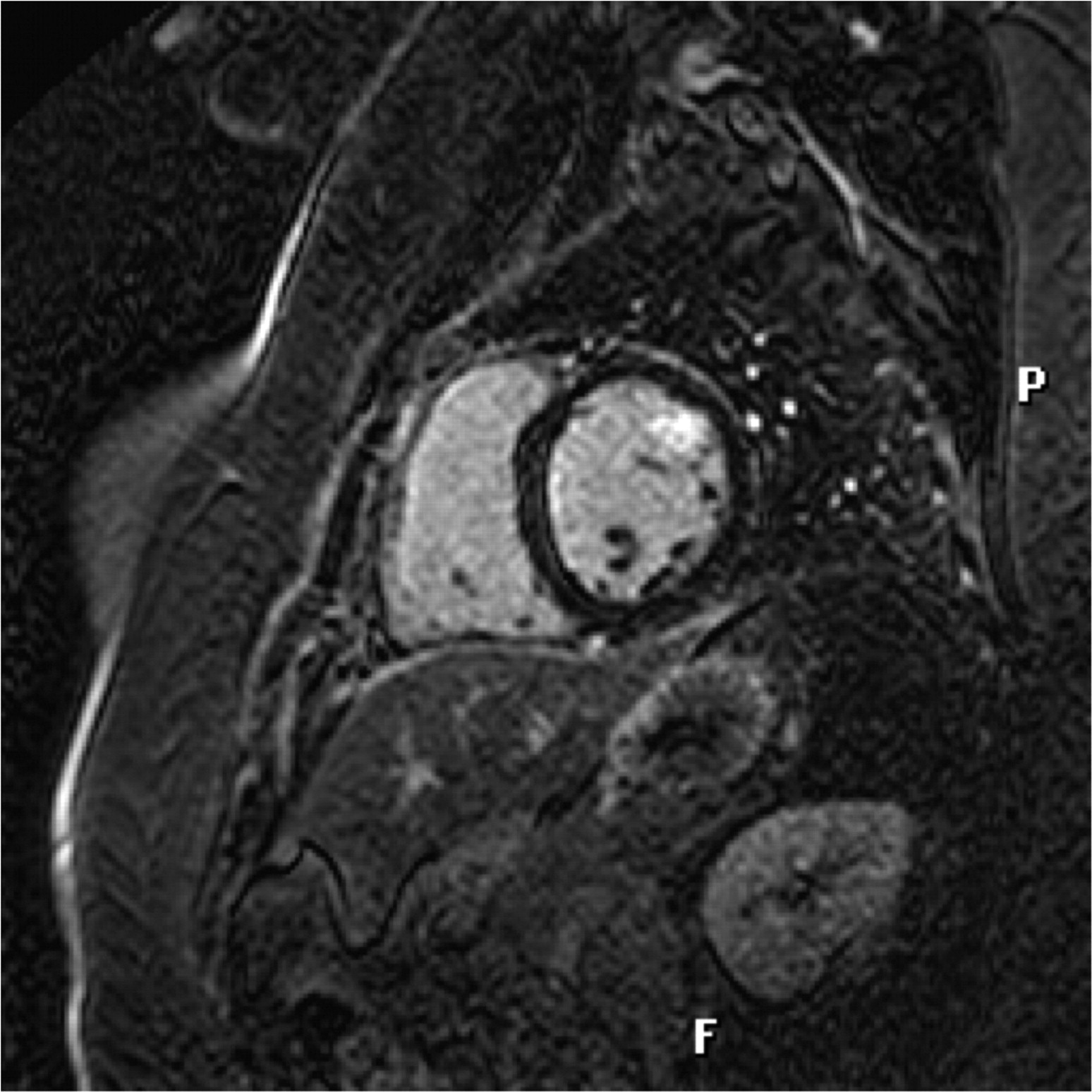
Cardiac MRI shows contrast enhancement of the anterolateral papillary muscle.
Due to recurrent ventricular tachycardia despite antiarrhythmic therapy and a concern for malignant primary cardiac tumor, the patient underwent a complete excision of the papillary muscle mass with mechanical mitral valve replacement. Cryoablation was performed as a box lesion around the stalk of the papillary muscle. Histopathologic evaluation of the 3.5 × 2.5 × 1.9 cm specimen (Figure 4) revealed myocardial tissue with extensive chronic inflammation and necrosis, of both infarctive and necrobiotic types. There was an associated granulomatous response with multinucleated giant cells. Extensive necrosis of the papillary muscle with associated arteritis was demonstrated by elastin staining (Figure 5). Stains for fungi and acid-fast bacilli were negative. Laboratory testing was negative for antineutrophil cytoplasmic antibodies, antinuclear antibodies, rheumatoid factor, and antistreptolysin O titer, and revealed a normal angiotensin-converting enzyme level. A final diagnosis of limited Wegener’s granulomatosis was made. The patient had an uncomplicated postoperative course and was discharged home in good condition. Serial imaging has been performed in concert with close rheumatologic followup with no evidence of localized or systemic disease progression.
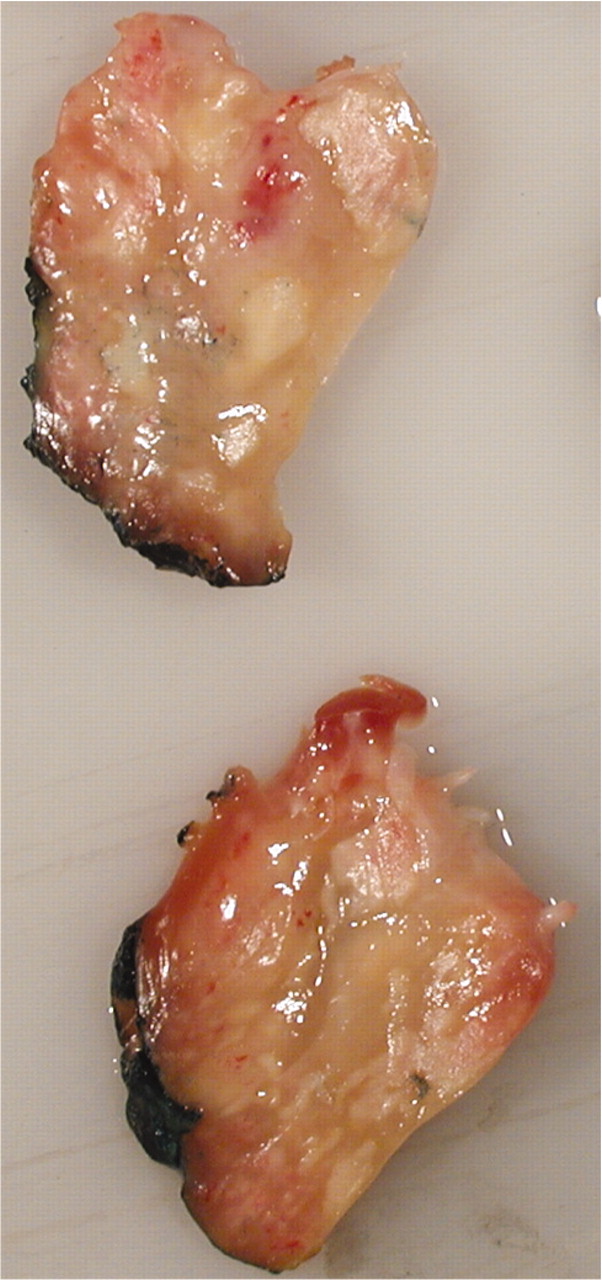
Gross pathologic specimens at time of surgical resection.
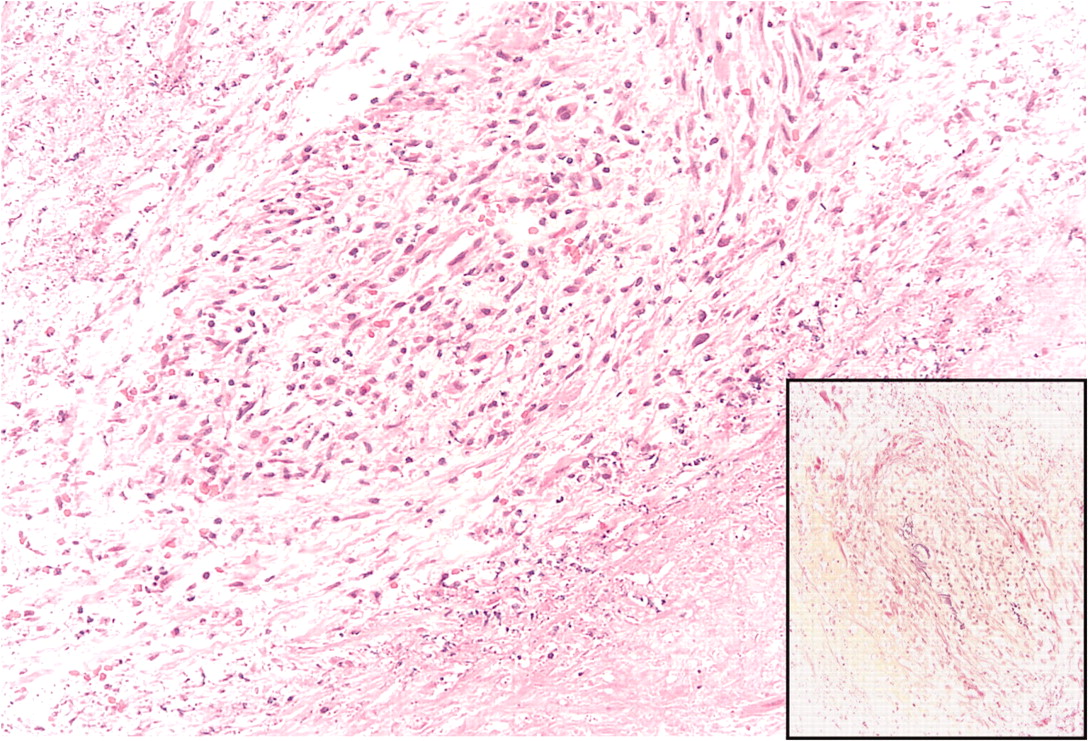
Histopathology reveals granulomatous inflammatory response with necrosis. Inset: Elastin staining confirms arteritis.
This case highlights an unusual presentation of localized vasculitis, isolated to the heart, and masquerading as a cardiac tumor. In this patient, use of her 12-lead electrocardiogram revealed a morphology and axis of the ventricular tachycardia that was consistent with a localization from the region of the anterolateral papillary muscle. Right bundle branch QRS morphology with inferior axis is characteristic of this location, and negativity in leads I and avL suggested a lateral wall site of origin1. Primary tumors of the heart are often distinctly separate from endocardial structures, and infiltrating or inflammatory disorders usually have other systemic findings. Although myxoma is the most common cardiac tumor, they are most frequently located adjacent to the interatrial septum in the left atrium. The most common primary cardiac malignancies are lymphomas and sarcomas2. In contrast to other sarcomas, rhabdomyosarcoma was considered in this case because it does not have any chamber predilection and can occur in young patients. Comparison of T1 and T2 intensity on MRI can be helpful in narrowing the differential diagnosis for primary cardiac tumors. In this case, the isointensity on T1 and hyperintensity on T2 weighted imaging was concerning for rhabdomyosarcoma. Additionally, the presence of necrosis can suggest fibrosarcoma or rhabdomyosarcoma3.
Inflammatory disorders that can involve the papillary muscles include sarcoidosis, Takayasu’s arteritis, Churg-Strauss, and Wegener’s granulomatosis4–8. MRI has been shown to be helpful not only in the diagnosis of Churg-Strauss, but also to monitor myocardial response to immunosuppressive therapy9. Cardiac involvement is rare in Wegener’s granulomatosis, occurring in approximately 6% of patients10. Pericarditis is the most common cardiac manifestation, although several case reports of arteritis and valvular lesions that mimic endocarditis and tumors have been reported11–13. A negative antineutrophil cytoplasmic antibody finding is consistent with extremely localized disease without systemic involvement.
To our knowledge, this is the first case to demonstrate localized Wegener’s granulomatosis of the papillary muscle.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}