

Abstract
Objective. To study the predictive value of antinuclear autoantibody (ANA) tests and antihistone antibodies (AHA) as risk factors for development of chronic asymptomatic uveitis of insidious onset in juvenile idiopathic arthritis (JIA).
Methods. ANA by indirect immunofluorescence using HEp-2 cells (IF-ANA), ELISA for ANA (E-ANA), and AHA were analyzed in sera of 100 children with recent-onset JIA and in 58 control sera. Clinical features, including age at onset, JIA subgroup, and presence of uveitis, were recorded in this prospective population-based cohort study.
Results. E-ANA was positive in 4 of the 100 sera, and was not associated with uveitis. Chronic uveitis developed in 16 children with JIA: in 14 of 68 positive for IF-ANA ≥ 80, and in 13 of 44 positive for AHA ≥ 8 U/ml. IgM/IgG AHA were found in higher proportions in children with uveitis (mean 12.4 U/ml) than in those with JIA and no uveitis (mean 6.9 U/ml) or in healthy controls (mean 4.3 U/ml).
Conclusion. No association was found between E-ANA and uveitis, and most IF-ANA-positive sera were E-ANA-negative. E-ANA is not clinically relevant in this setting and should never be used to determine frequencies of eye examinations to detect new uveitis in JIA. AHA ≥ 8 U/ml, IF-ANA titer ≥ 320, and young age at onset of arthritis were significant predictors for development of chronic uveitis. The diagnostic value of AHA ≥ 8 U/ml as a biomarker of chronic uveitis in JIA is very similar to IF-ANA ≥ 80.
Juvenile idiopathic arthritis (JIA) is the most common rheumatic disease of childhood, and this diverse clinical entity of arthritis in children is believed to be of largely autoimmune origin. Over the last decade the International League of Associations for Rheumatology (ILAR) classification system has been accepted worldwide as a useful tool to describe the umbrella term JIA1. Efforts to validate and improve the classification of chronic childhood arthritis are continuing. Recently, circulating antinuclear antibodies (ANA) have been suggested as a possible modifier of the current ILAR classification system of JIA2.
Convincing data for a role of ANA in the pathophysiology of JIA are lacking, but presence of ANA detected by immunofluorescence is reported to be an important risk factor for development of uveitis3. Uveitis occurs in 10%–20% of children with JIA. The uveitis in JIA is most often chronic and asymptomatic, and may lead to reduced vision or blindness4,5. Regular slit-lamp examination at specific intervals in the followup of all children with JIA is therefore important6. Different screening programs are published based on certain risk factors, such as presence of ANA, oligoarticular subtype, female sex, and young age at onset of arthritis3,7–9. According to the American Academy of Pediatrics guidelines, a negative ANA status leads to increased interval between eye examinations for detecting newly developed uveitis3.
The presence of ANA in JIA is traditionally detected by an indirect immunofluorescence method using HEp-2 cells (IF-ANA) and is reported in 6%–65% of children with JIA10–12. This method has been criticized for operator-dependency and lack of specificity. Positive IF reactions are frequently due to autoantibodies against nuclear antigens that are poorly identified and not known to be associated with specific clinical conditions. ELISA enables automated identification of antigen-specific ANA13. These ELISA utilize well defined nuclear antigens selected for identifying autoantibodies with strong associations to specified systemic autoimmune diseases. Previous studies have shown that ELISA ANA (E-ANA) techniques detect fewer ANA in children with JIA than the IF-ANA technique does10,14.
The antigenic specificity of ANA in JIA has not been elucidated, but antibodies to histones, non-histone chromatin, and a 45-kDa DEK nuclear antigen are reported to be present in subsets of children with JIA15–17.
Histones are basic DNA-binding proteins that are subcomponents of chromatin, and the core histones are evolutionarily highly conserved between species15. Antihistone antibodies (AHA) are found associated with drug-induced systemic lupus erythematosus (SLE) and a variety of other adult autoimmune diseases15,18. AHA have been found in juvenile arthritis and in some studies were associated with early-onset disease, oligoarticular onset, and uveitis16,19–21, whereas others have found no such association22–25. Studies on AHA, the 5 histone subtypes, and histone peptides show considerable discrepancies, probably due to the variety of substrates and test systems used such as immunoblotting and different ELISA15. There is no consensus whether histone should be part of the antigen mixture in E-ANA.
The increasing use of E-ANA tests in immunological laboratories13,26,27 calls for a thorough investigation and discussion of the clinical implications of the different methods in children at risk of JIA-associated uveitis. Our aim was to evaluate the value of ANA, analyzed by ELISA and IF techniques, and of antihistone antibodies in predicting chronic uveitis in patients with newly diagnosed JIA in a prospective longitudinal cohort study.
MATERIALS AND METHODS
Patients
We prospectively included consecutive patients with newly diagnosed JIA from 5 counties in the middle and northern parts of Norway, from 1997 to 2002. The incidence of JIA in the study area in 1997–98 was 22.4 per 100,000 children28. During the study period, 174 patients with a diagnosis of JIA were registered and asked if they would give permission to draw a blood sample and participate in the study. All patients who accepted and had a blood sample taken within a year of diagnosis, and with a stored serum volume sufficient for analysis of IF-ANA, E-ANA, and AHA, were included, giving 100 participants. Of the 74 children that were excluded from the study, 6 did not give written consent, 1 had bilateral anophthalmia, and 67 patients did not have sufficient blood volume stored. Family history and extensive clinical information, including occurrence of uveitis, number of affected joints, systemic symptoms, enthesitis, and psoriasis were registered at baseline and at 1- to 2-year intervals. HLA-B27 was analyzed at onset, and rheumatoid factor analyzed twice, at least 3 months apart. JIA subtypes were determined according to the ILAR criteria, based on all available information that was registered within 1 year of disease onset1. Uveitis was described in terms of presence of symptoms, duration, and course of uveitis in the database, and retrospectively classified according to the recommendations by the Standardization of Uveitis Nomenclature (SUN) working group29. Uveitis was then defined as “acute,” symptomatic with acute onset and limited duration, or “chronic” insidious onset, mainly asymptomatic with chronic recurrent or persistent course. Control sera were collected in order to provide information on the presence of E-ANA, IF-ANA, and mean serum values of AHA in a healthy childhood population. The control sera were obtained from routine blood tests in 58 children, with no diagnosis of inflammatory diseases, undergoing elective outpatient procedures. The Regional Committee for Medical Research Ethics and the Norwegian data authorities approved the study. Informed consent was obtained from parents of children aged < 16 years and from the children themselves if aged ≥ 16 years.
Serology
The serum samples were frozen and stored at −70°C in aliquots to avoid repeated freeze-thaw cycles. A conventional ANA indirect immunofluorescence assay (IF-ANA) was performed (St. Olavs Hospital, Trondheim, Norway). The sera were screened at 1:80 dilution in phosphate buffered saline, using HEp-2 cell slides (Immunoconcepts, Sacramento, CA, USA). The IF-ANA slides were scored positive by microscopy if there was a clearly discernible pattern of nuclear fluorescence at 100× unfiltered magnification. All tests were scored blindly and independently by 2 experienced laboratory medical technologists. A few discrepant conclusions were settled by joint reexamination. For titration, sera that screened IF-ANA-positive were frozen, and later thawed and retested at dilutions 1:80, 1:320, 1:1280, and 1:5120, and the IF-ANA-pattern was described.
E-ANA screening of the JIA sera was performed at 1:101 dilution using an ELISA kit encompassing the following recombinant or purified native nuclear antigens: ds-DNA, U1RNP, Sm, Ro/SSA (52-kDa, 60-kDa), La/SSB, Scl-70, CENP-B, and Jo-1 (Varelisa Recombi ANA Screening test from Pharmacia Diagnostics, Freiburg, Germany). Positive screening was followed by retesting using a multiplex Luminex kit, and testing simultaneously for specific antibodies to the following antigens: ds-DNA, SSA (60-kDa), SSA (52-kDa), SSB, Sm, Sm/RNP, Scl-70, Jo-1, centromere, and ribosome (FIDIS Connective10 from Biomedical Diagnostics, BMD France, Marne-la-Vallée, France).
AHA were detected with a Varelisa Histone Antibodies EIA kit (Pharmacia Diagnostics) at the University of Tromsø. The sera were first tested for antihistone IgG using an IgG conjugate, and then for antihistone IgM/IgG using a combined IgM/IgG conjugate. The manufacturers’ suggestions for quantitative evaluation of test results were followed; < 30 U/ml was considered negative while serum levels ≥ 30 U/ml were considered positive. The ELISA tests for ANA and AHA and the Luminex test for extractable nuclear antigens (ENA) were run according to the manufacturers’ instructions in detail.
Analytical procedures and statistical methods
Statistical analyses were performed using the Stata version 10 software (Stata Corp., College Station, TX, USA). The chi-squared test was used as appropriate for comparison of dichotomous variables. The Student’s t-test and analysis of variance, with Bonferroni contrasts, were used to compare means in continuous outcomes between groups, logarithmic transformation of the variable was carried out, and geometric means reported for skewed data when appropriate. Odds ratios (OR) with 95% confidence intervals (CI) were calculated using logistic regression. The p value < 0.05 was considered significant. Sensitivity, specificity, the likelihood ratio (LR), and the positive and negative predictive values were calculated for potential clinical and serologic markers of uveitis, to describe the test performances. In all the analyses of these biomarkers the children with chronic uveitis have been compared with children without chronic uveitis. The receiver-operating characteristics (ROC) curve was used to compare AHA and IF-ANA as predictors of uveitis, and to assess the sensitivity and specificity of different cutoff levels of AHA. The ROC curve is a plot of sensitivity against (1 – specificity) for different choices of test cutoff. An indifferent test has an area under the curve (AUC) of 0.5, and the perfect test an AUC of 1. The best predictor is the test with the highest AUC.
RESULTS
Clinical data
Of the 100 children with JIA, 71 were girls, and 50 were classified as persistent or extended oligoarticular subtype according to the ILAR criteria. There were no statistically significant differences in the incidence of uveitis or in the proportion of children with persistent or extended oligoarticular ILAR subtype among the cohort of all children with JIA (n = 174) and study participants with an available serum sample (n = 100). Median age at onset of arthritis was 5.3 (range 0–15) years. During a mean observation time of 7 (range 3–11) years, 18 of the children developed uveitis (Figure 1). Two children with enthesitis-related arthritis had acute symptomatic uveitis of sudden onset, and the remaining 16 had chronic, mainly asymptomatic, uveitis of insidious onset. The control group of healthy children had a median age of 6 years (range 8 months-14 yrs) and 50% were girls.

Proportion of children developing chronic asymptomatic uveitis (n = 16) over time after onset of arthritis in a cohort of 100 patients with juvenile idiopathic arthritis. Two patients had uveitis diagnosed before onset of arthritis.
Antinuclear antibodies
Of the 100 patient sera, 4 were E-ANA screening-positive, whereas 68 were positive using the IF-ANA screen test (Table 1). Titration of the IF-ANA screen-positive sera showed IF-ANA ≥ 80 for 57 sera. Anti-ENA were detected in 3 of the E-ANA-positive sera: anti-ds-DNA, anti-Scl-70, and anti-SS-A52. The IF-ANA pattern was described as homogeneous or partly homogeneous in 86% of the IF-ANA-positive patient samples (data not shown). Among the control sera, 7 of 58 were IF-ANA-positive, and no E-ANA positivity was found (Table 1). Uveitis developed in 14 of the 68 IF-ANA-positive patients, but in none of the 4 E-ANA-positive patients (Figure 2).
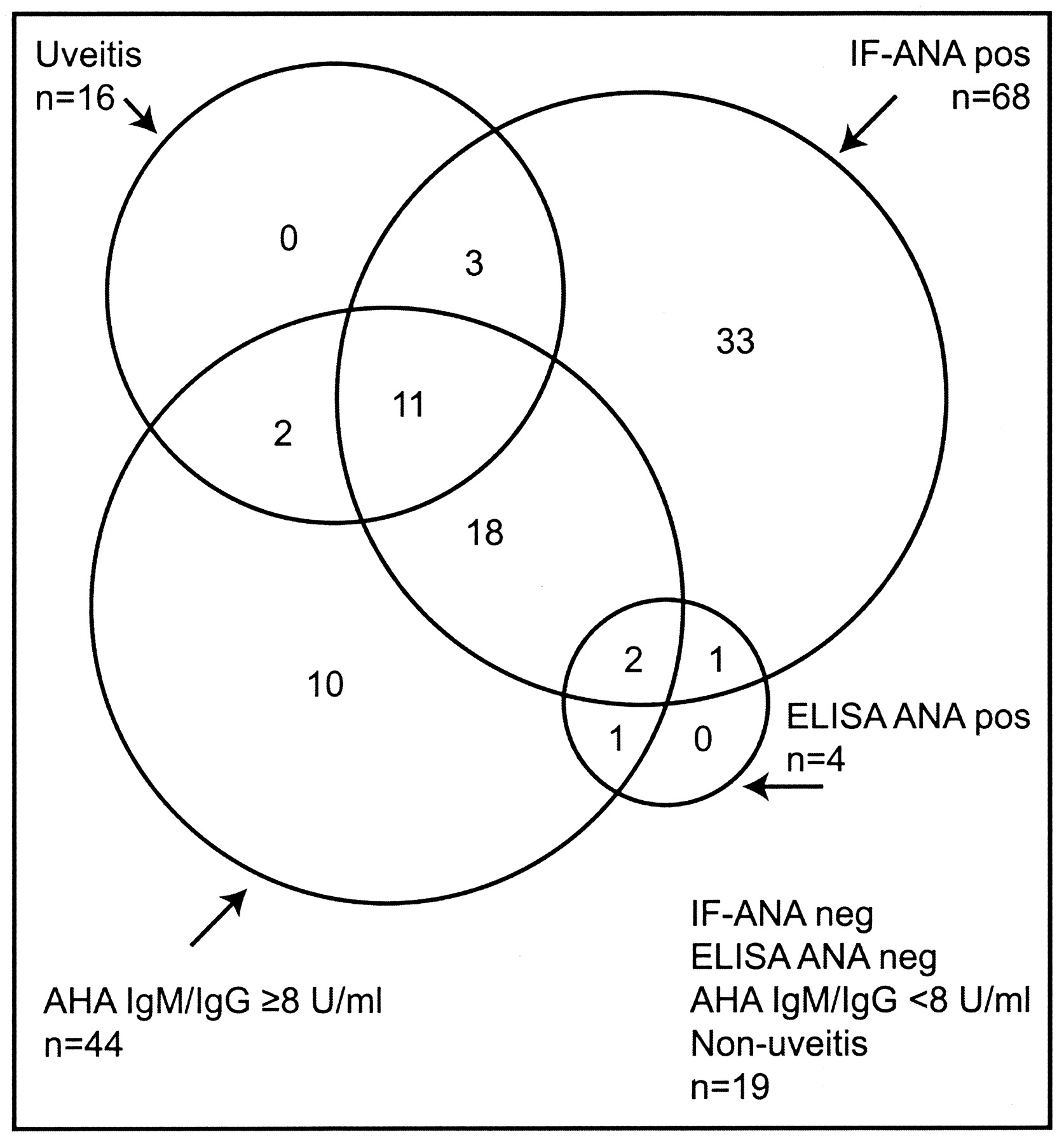
Prevalence and agreement between chronic asymptomatic uveitis and sera positive for immunofluorescence using HEp-2 cells (IF-ANA), ELISA ANA, and antihistone antibodies (AHA) IgM/IgG ≥ 8 U/ml in 100 children with recent-onset juvenile idiopathic arthritis.
Biomarkers present in sera of 100 Norwegian children with recent-onset juvenile idiopathic arthritis (JIA) and 58 healthy children.
Antihistone antibodies
Antihistone IgM/IgG was found in 6 of the 100 children with JIA, and in 1 of the 58 healthy controls (cutoff 30 U/ml; Table 1). AHA IgM/IgG was significantly associated with development of uveitis, as 4 of the 16 children with chronic uveitis were AHA-positive compared to 2 of 84 without uveitis (Table 2). Mean AHA IgM/IgG was 12.4 U/ml in JIA children with uveitis, 6.9 U/ml in children without uveitis, and 7.6 U/ml in all children with JIA. In sera from healthy controls, mean AHA IgM/IgG was 4.3 U/ml. There was a statistically significant difference in mean AHA serum levels between JIA children with and without uveitis (p = 0.012), between children with uveitis and healthy controls (p < 0.0001), and between children with JIA and healthy controls (p < 0.0001). There were no significant differences in sera testing AHA IgM/IgG ≥ 8 U/ml between JIA subgroups.
Odds ratios (OR) for development of chronic asymptomatic uveitis in 100 Norwegian children with recent-onset juvenile idiopathic arthritis (JIA), based on analyses of clinical and biological characteristics.
Predictors of chronic asymptomatic uveitis
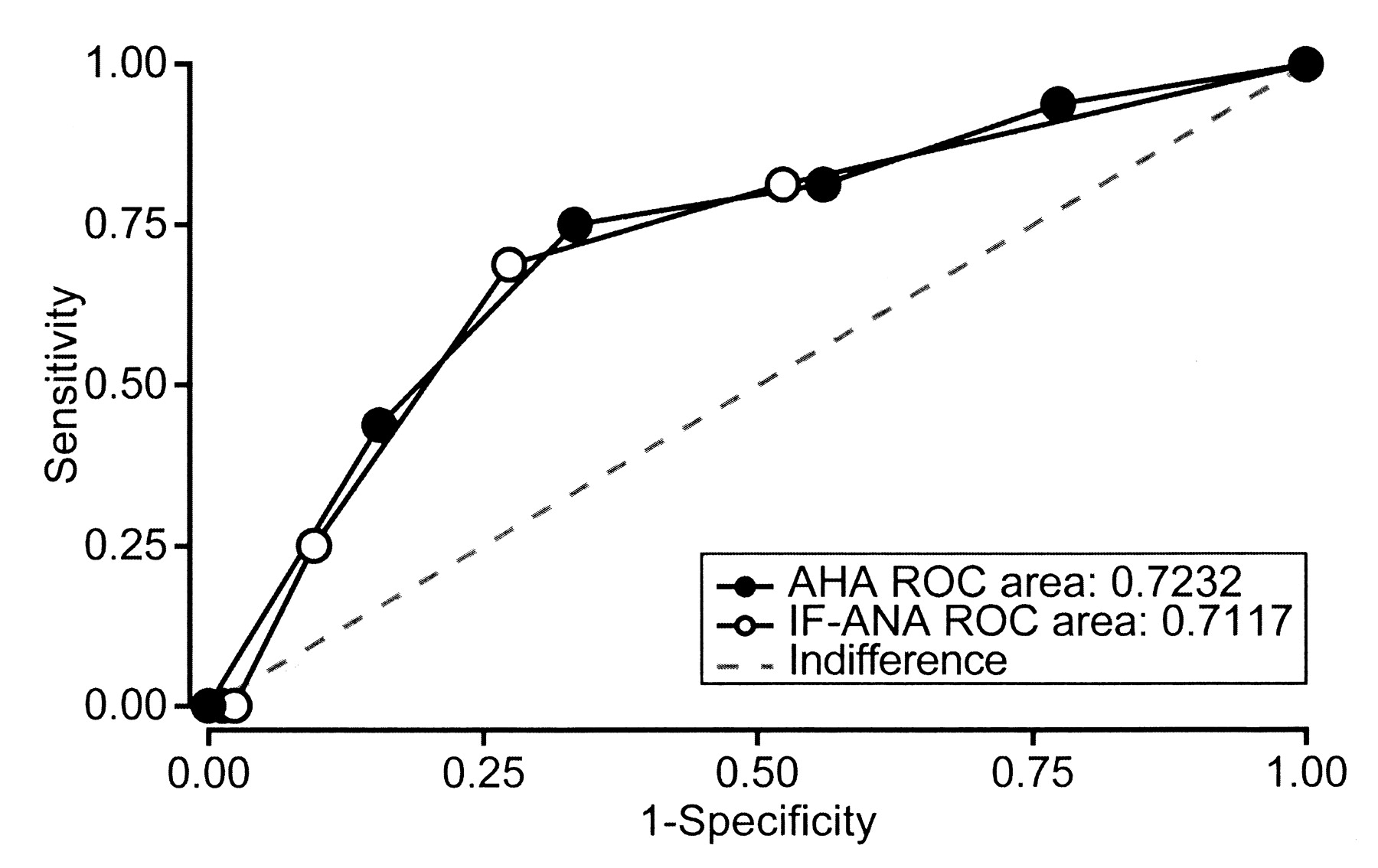
Clinical and serological variables previously reported to be associated with uveitis were evaluated as predictors of chronic asymptomatic uveitis (Tables 2 and 3). Young age at onset of arthritis, the presence of IF-ANA titer ≥ 320, and antihistone IgM/IgG ≥ 30 U/ml were significantly associated with the development of uveitis. The ROC curve of antihistone IgM/IgG, as a predictor of uveitis, shows an AUC of 0.72 [standard error (SE) = 0.07] and for IF-ANA of 0.71 (SE = 0.07; Figure 3). Assessing different cutoff values of AHA using the ROC curve (Figure 3), AHA IgM/IgG ≥ 8 U/ml was found to identify 13 of the 16 patients who developed chronic uveitis, showing a significant association between AHA and uveitis (OR 7.4, 95% CI 2.0–28.0; Table 2). AHA IgG ≥ 5.5 U/ml and IF-ANA ≥ 320 each identified 11 of the 16 patients developing uveitis (Table 2). The relation between chronic uveitis and sera positive for IF-ANA, E-ANA, and AHA IgM/IgG ≥ 8 U/ml is shown in Figure 2. All children with JIA who developed chronic uveitis had sera positive for IF-ANA ≥ 80, or AHA IgM/IgG ≥ 8 U/ml, or both. Analysis of the test properties of AHA IgM/IgG ≥ 8 U/ml, as a predictor of uveitis, shows higher specificity, positive and negative predictive values, and likelihood ratios, and the same sensitivity as IF-ANA titer ≥ 1/80 with respect to uveitis (Table 3).

Receiver-operating characteristics (ROC) were used to examine the test properties of IF-ANA titer (< 80, 80, 320, 1280, 5120) and serum level of antihistone antibodies (in quintiles: < 4.1, 4.1–6.2, 6.3–8.4, 8.5–12.0, > 12.0 U/ml) as predictors of uveitis in juvenile idiopathic arthritis.
Test performance of potential clinical and biological predictors of chronic asymptomatic uveitis in 100 Norwegian children with recent-onset juvenile idiopathic arthritis (JIA).
DISCUSSION
Our results demonstrate no clinical effect of E-ANA in JIA. The main clinical application of ANA in JIA is risk stratification for the frequency of eye examinations for detecting chronic asymptomatic uveitis. Previous reports on ANA as a predictor of uveitis in JIA are based on the IF-ANA method4,8,30. In agreement with the findings of Reiff, et al10, most IF-ANA-positive sera in our study were E-ANA-negative. Further, no children developing uveitis in our study were E-ANA-positive. Clinicians must be cautioned not to make decisions on less frequent ophthalmologic examinations in patients with JIA based on a negative ANA performed by the ELISA technique. The lack of association between E-ANA and uveitis in children with JIA is clinically important and, to our knowledge, has not previously been reported.
ANA detected by ELISA is increasingly used due to its ability to detect the clinically relevant ANA in adults13, a higher cost-effectiveness, and standardization as a result of operator-independent automated analyses. Several different commercially available ANA ELISA, including recombinant antigens, have been tested in children with JIA and in juvenile SLE and healthy controls10,14, showing no association with IF-ANA, which suggests lack of incorporation of antigens relevant to children with JIA. Inconsistent results between ELISA with significant test-to-test variability have also been reported14,31. Our study adds evidence to the conclusion of these previous reports, that E-ANA is not useful for the detection of clinically relevant ANA in JIA.
Our study shows that AHA are found in higher proportions in children with JIA-associated uveitis than in children with JIA and no uveitis or in healthy controls, and constitute a significant and independent biomarker for development of uveitis in JIA. In healthy adults equally distributed by sex and age, the manufacturers report that AHA IgM/IgG is present at mean values of 9.5 U/ml32. In our study, a mean value of 4.3 U/ml was found in the control sera from children with no inflammatory diseases, indicating lower normal values in healthy children than in adults. A high proportion of the control sera had AHA IgM/IgG ≥ 8 U/ml (Table 1); however, the differences in mean AHA serum levels between JIA children with and without uveitis and healthy controls were all statistically significant. The results indicate a predictive value of AHA levels in discriminating between uveitis and non-uveitis in children with an established diagnosis of JIA, even in the range of “normal” adult serum levels. The AHA ELISA was designed to aid in the diagnosis of drug-induced lupus erythematosus and SLE32. As a predictor of uveitis in JIA, different cutoff levels may be more appropriate.
The consequences of delayed diagnosis and treatment of uveitis may be serious4,33. Useful predictors of uveitis must therefore identify as many as possible of the children with JIA who eventually develop uveitis. IF-ANA ≥ 320 and AHA ≥ 30 U/ml show a high specificity, but sensitivity that is too low to find children at risk. IF-ANA screening at titer ≥ 80 shows a low specificity, including 68 of the 100 children, but identifies 14 of the 16 children with asymptomatic uveitis. AHA IgM/IgG ≥ 8 U/ml identifies 13 of the 16 children with asymptomatic uveitis. AHA IgG ≥ 5.5 also shows a significant association with asymptomatic uveitis. AHA IgM was not analyzed separately in our study. Compared to IF-ANA ≥ 80, our data suggest that AHA IgM/IgG ≥ 8 U/ml has the same sensitivity, better predictive value, and higher likelihood ratio as a biomarker of asymptomatic uveitis in JIA.
The presence of AHA in juvenile arthritis and the association with uveitis have been found in previous studies, AHA being predominantly of the IgM subtype16,19,20,34. Other studies, however, show no association between AHA profile and uveitis22–24. Most groups performed analyses of only IgG antibodies against the different histone classes (H1, H2A, H2B, H3, and H4) and histone peptides. Ostensen, et al20 found a higher frequency of H3-reacting antibodies in children with juvenile chronic arthritis and chronic anterior uveitis compared to children with no eye disease. None of the previous studies has been population-based with consecutive patient recruitment or used the ILAR classification in recruitment and subgrouping of the patients. The timepoint of blood sampling early in the disease course may be of importance and partly explain the discrepancies in results.
Our study is strengthened by its prospective design, while small numbers may be a weakness. Other studies on ANA and AHA in JIA and uveitis are based on comparable or smaller patient populations19–24, and in spite of limited observation time and number of uveitis cases, the prevalence of uveitis of 18% is comparable to other Nordic studies with longer followup35,36. The proportion of children with persistent and extended oligoarticular JIA was comparable to other population-based studies. Measures were taken to avoid repeated freeze-thaw cycles of the sera, but the IF-ANA tests were performed twice and 11 of the 68 IF-ANA screen-positive sera had IF ANA < 80 on the following titration.
Recent studies reporting a declining trend in complications of uveitis in JIA indicate that early detection and prompt treatment are essential for visual outcome6,33,36. Clinical and biological predictors of uveitis defined as early as possible after onset of arthritis are valuable in risk stratification before deciding on frequency of eye examinations. In agreement with our study, young age at onset of arthritis is consistently reported to be the most important predictor of uveitis4,7,8,30. In line with Kotaniemi, et al4 and Reininga, et al7, we found female sex not to be associated with uveitis, in contrast to many earlier studies. Reininga, et al also reported that IF-ANA was not associated with uveitis, and even that ophthalmologic complications were more common in children with uveitis and JIA who were IF-ANA-negative7. Ophthalmologic examination guidelines independent of serologic biomarkers may be the safest option, with increased frequency the first 4 years of JIA when 90% of uveitis develops4,7,9.
ANA detected by ELISA technique is of no clinical significance in JIA and should never be used as a guide to decide frequencies of eye examinations. AHA seem to be significantly associated with a risk of developing uveitis in JIA, with test performances similar to or, in some aspects, better than IF-ANA. A combination of AHA and IF-ANA may be of clinical value, because all children with chronic uveitis in our study were positive in one of the 2 tests. Further studies are needed to confirm the clinical utility of AHA or the combination of ANA/AHA in predicting uveitis in JIA. The role of any serologic marker in determining the frequency of eye examinations for detecting silent uveitis in children with JIA can be questioned, and the implication of ANA tests in this setting is highly dependent on the method.
Acknowledgments
We thank the children and parents participating in the study. We thank the Nordic Study group of Pediatric Rheumatology (NoSPeR); Prof. Gudmund Marhaug in Trondheim, Prof. Freddy Karup Pedersen, Drs. Susan Nielsen and Marek Zak in Copenhagen, Drs. Pekka Lahdenne and Kriistina Aalto in Helsinki, Prof. Anders Fasth in Gothenburg, and Dr. Boel Anderson-Gäre in Jonköping for inspiring cooperation. We thank Kirsten Nilsen and Oddrun Storrø for well performed technical assistance, Drs. Astri Lang and Anne Elisabeth Ross in Tromsø, and Drs. Kjell Berntzen and Nina Moe in Trondheim for collecting data. We thank Prof. Ole Petter Rekvig for interesting discussions and valuable critical review of the manuscript.
Footnotes
-
Supported by grants from the Grete Harbitz Foundation and the Helse Nord Research Program.
- Received July 1, 2009.
- Accepted for publication March 12, 2009.








{kind=link}
{kind=link}
{kind=link}