
The classification of juvenile inflammatory arthritis (JIA) has been formulated against the well established dogma that pediatric “inflammation against self” is autoimmune in origin. Given that adult rheumatoid arthritis (RA) is a paradigm of such autoimmune disease, this comparator benchmark has been used for the categorization of the JIA spectrum of joint disease. Consequently, the etiopathogenesis of joint inflammation in polyarticular and oligoarticular JIA has been considered mostly in relationship to synovial-based disease. This includes the synovium that lines diarthrodial joints, but also synovium associated with bursae and tendon sheaths.
In this issue of The Journal, Rooney and colleagues present a cross-sectional study in JIA patients with active, ankle-based disease using sonography to delineate the precise anatomical distribution of joint inflammation1. Specifically, they asked whether ankle joint swelling that was regarded as clinically significant affected the ankle joint itself, the tendons crossing the ankle joint, or both. The primary impetus for this work was to determine whether clinical assessment of disease with respect to anatomical territory involvement as joint cavity-based or tenosynovial-based was accurate.
A better understanding of the precise localization of inflammation could have important implications for local steroid injection therapy in such cases. However, the authors did not attempt to specify which particular tendons were involved and in relation to which bony prominences — other than a passing reference to tibialis posterior (which uses the medial malleolus as a pulley in its journey between the leg and foot2).
In a cohort of 34 children with 49 swollen ankle joints where the swelling was deemed to be centered on the ankle joint proper, the authors made the following observations: the commonest abnormality overall was tenosynovitis, being present in 71% of cases. What was more surprising was that tenosynovitis as a sole abnormality was present in 39% of cases. When ankle disease was stratified, it was noted that the oligoarticular JIA group exhibited tenosynovitis without tibiotalar involvement much more commonly than the polyarticular group (56% vs 29%, respectively). Moreover, medial ankle tenosynovitis was observed in 81% of oligo-JIA group ankles, compared to 52% with poly-JIA ankles. However, lateral ankle joint tenosynovitis (i.e., that which must have been associated with the tendons of peroneus longus and brevis) was rare in oligoarticular JIA, but common in polyarticular JIA.
This is a fairly small study, and further confirmatory work is needed, including intraobserver work and a more detailed analysis to determine which tendons are involved and at precisely what sites. Recruitment of an inception cohort with longitudinal followup is needed, and close correlations with other JIA disease features including antinuclear antibody positivity are needed to better explore these phenotypes if they are confirmed. In studies comparing the pattern of disease with adult rheumatoid factor- and anti-cyclic citrullinated peptide antibody-positive RA it may also be relevant to prove if ankle joint disease actually has different patterns.
That being said, the study of Rooney, et al has 2 equally important implications, one clinically oriented and of immediate relevance and the other of potential relevance to a better understanding of disease pathophysiology. The clinical slant to this work is self-evident: ultrasound could be useful in guiding local steroid injection. The value of such an approach now needs to be assessed in a prospective study.
The remainder of this commentary discusses the possible predilection for tendon disease in the ankles in oligoarticular JIA and what this could mean. In particular we would emphasize that tendon disease does not necessarily imply autoantibody-related synovial autoimmunity. In the last decade we provided a microanatomical explanation for tenosynovitis in relation to the seronegative spondyloarthropathies3. At locations where tendons change direction and wrap around bony pulleys in the ankle region (which include not only the malleoli but also the sustentaculum tali and the peroneal tubercle2) both the tendon surface in contact with the bone and the bone itself are fibrocartilaginous4 (Figure 1). These cartilages are strategically located to minimize mechanical stressing and thus “wear and tear” at sites of shearing and compression. This is a consequence of the longitudinal excursion of tendons as muscles contract and the “pulley-rope”-like relationship between bone and tendon. Tendons at these locations have long been called “wraparound tendons” (a term popularized by the pioneering work of Kate Vogel and colleagues5). However, as these are prone to inflammation in the seronegative spondyloarthropathies, we have likened the tendon-bone association to functional entheses — signifying that, as at a true enthesis, there is tendon-bone contact, even if the former does not attach to the latter3. It is thus worth noting that the magnetic resonance image appearance of “wraparound tendon disease” at the ankle is associated with a diffuse osteitis in the adjacent bone6, i.e., recalling the pattern of abnormality associated with enthesitis-related pathology elsewhere7.

{kind=link}
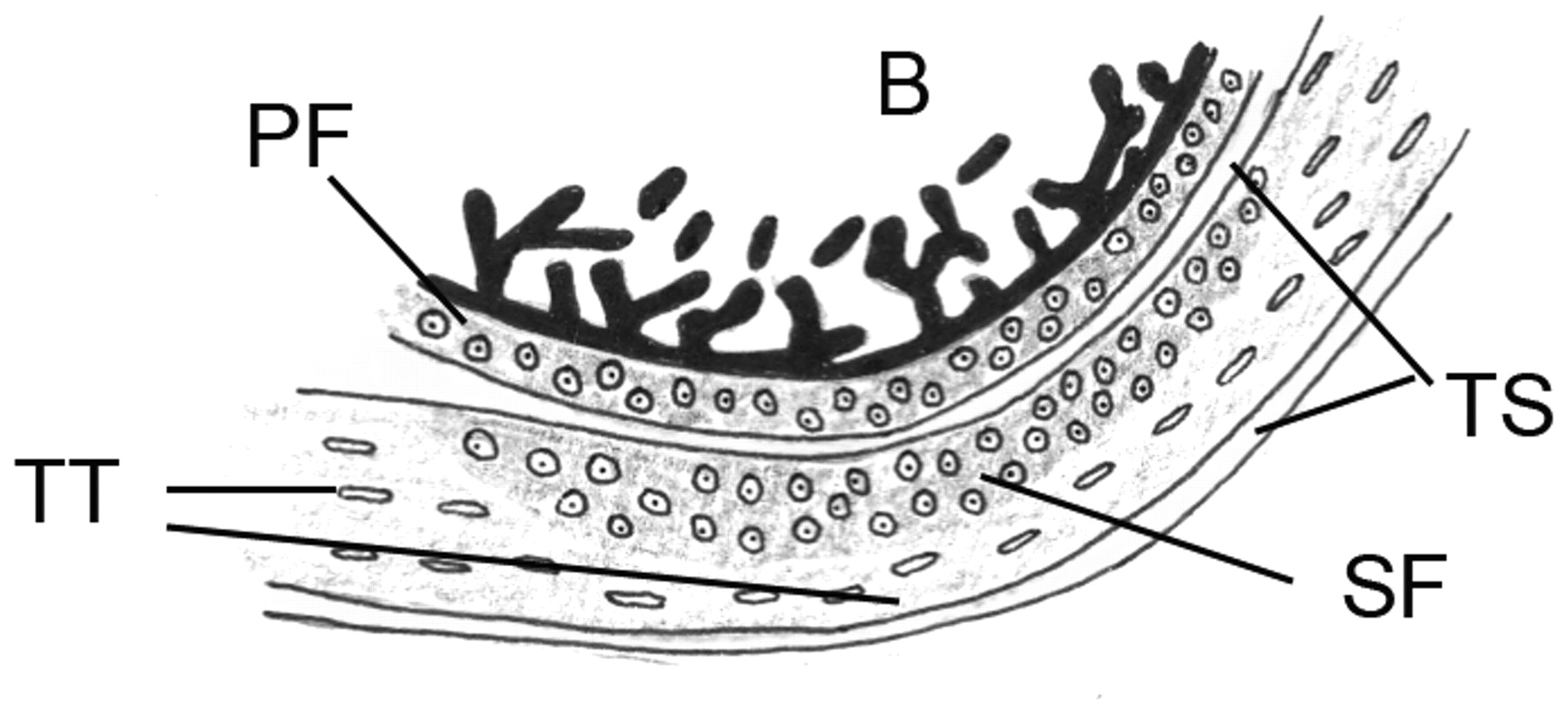
A representation of a “wraparound tendon” that forms a functional enthesis with the adjacent bony pulley, e.g., as in the region of the ankle malleoli. The periosteum shows evidence of fibrocartilage differentiation and is thus referred to as a periosteal fibrocartilage (PF) and the deep surface of the associated tendon has a sesamoid fibrocartilage (SF) near its deep aspect. However, both proximal and distal to the site of compression, and on the surface of the tendon facing away from the bone, typical “tensional tendon” (TT) is present. We believe that the high degree of stressing at such sites might lead to innate immune system activation at these sites and thus contribute to the patterns of JIA that are observed.
Why are these ultrasound and microanatomical observations potentially so important? It is of particular interest that both psoriatic arthritis and enthesitis-associated arthritis form part of the JIA spectrum. Both these arthropathies are intimately associated with iridocyclitis. It is also well known that the oligoarticular form of JIA is also associated with iridocyclitis. The possible link between tendon diseases in oligoarticular JIA in the present study raises the possibility of shared tissue microanatomical factors between the tendon and the eye. Common unifying factors including repetitive stressing, motion, and microdamage of these moving joint parts and ocular tissues have previously been suggested3,8.
The present findings and possible relevance of the tendon disease localization, particularly in oligoarticular JIA, take on increasing importance with the realization that autoimmunity as embodied by aberrant B and T cell responses is less likely to be the primary driver in many categories of JIA9 and in inflammation against self in general10. Given the relative rarity of JIA, academic pediatric rheumatologists need to collaborate to create inception cohorts and link baseline synovial and tendon-based disease to other features including antinuclear antibody status and uveitis. An understanding of the underlying joint and tendon physiology and why normal antiinflammatory homeostatic mechanisms may fail in JIA could be equally important. Linking these anatomical patterns of disease to the emerging genetic basis for inflammatory arthritis could also be key to genotype-phenotype correlations. Specifically, how these tissue-specific factors lead to regional innate immune activation could be key to a better understanding and classification of JIA, without assuming the classical autoimmune paradigm of JIA that applies to diseases that include seropositive RA9.
Footnotes
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.