

To the Editor:
Systemic sclerosis (SSc) is a complex autoimmune connective tissue disease characterized by cutaneous and visceral fibrosis and widespread vascular pathology1. Digital ulcers (DU) are a major clinical problem in SSc, occurring in about one-third of patients2. DU cause local pain and functional impairment and have a negative effect on quality of life for patients with SSc2. Therapeutic agents potentially used for management of DU include calcium channel blockers, α-adrenergic inhibitors, angiotensin II-converting enzyme inhibitors, prostacyclin analogs, phosphodiesterase-5 inhibitor, and others2. Bosentan is a specific orally active dual endothelin receptor antagonist that has been used for the treatment of pulmonary hypertension (PH) and recently for DU3–5. The objective of our study was to examine the effectiveness and safety of bosentan for healing DU in patients with SSc over the long term.
For a cohort of 110 patients with SSc, 30 patients with DU were identified. All patients fulfilled the American College of Rheumatology criteria for SSc6 and all were refractory to calcium channel antagonists, angiotensin II inhibitors, or sildenafil.
Patients were treated with bosentan 62.5 mg twice/day for the first month and 125 mg twice/day from the second month for a period of 36 months. The primary endpoints were the number of healed DU and the number of new skin ulcers formed. Pregnant women and nursing mothers and patients with liver or kidney disease, blood dyscrasias, diabetes mellitus, severe cardiopulmonary diseases, or scleroderma renal crisis were excluded from the study.
We gave patients a complete examination and measured the number of treated DU and new ulcers formed. More specifically, all ulcers were measured at entry and every 3 months thereafter for a period of 36 months. Skin biopsies of affected areas were performed in 5 patients, at the same place before and after therapy. From these 30 patients, 4 were excluded: 2 had abnormal liver function test, 1 had thrombocytopenia, and 1 had diabetes mellitus with liver steatosis. Thus, 26 patients were investigated. There were 22 women and 4 men with mean age of 60.0 ± 6.5 years and mean disease duration of 12.5 ± 8.6 years. Sixteen had limited scleroderma, while 10 had the diffuse type of the disease. Five patients had PH and 3 of them also had pulmonary fibrosis. Twenty were treated with methotrexate (0.2 mg/kg body weight) plus small doses of prednisone (< 7.5 mg/day), 3 with mycophenolate mofetil and small doses of steroids, and 4 with prednisone (< 7.5 mg/day).
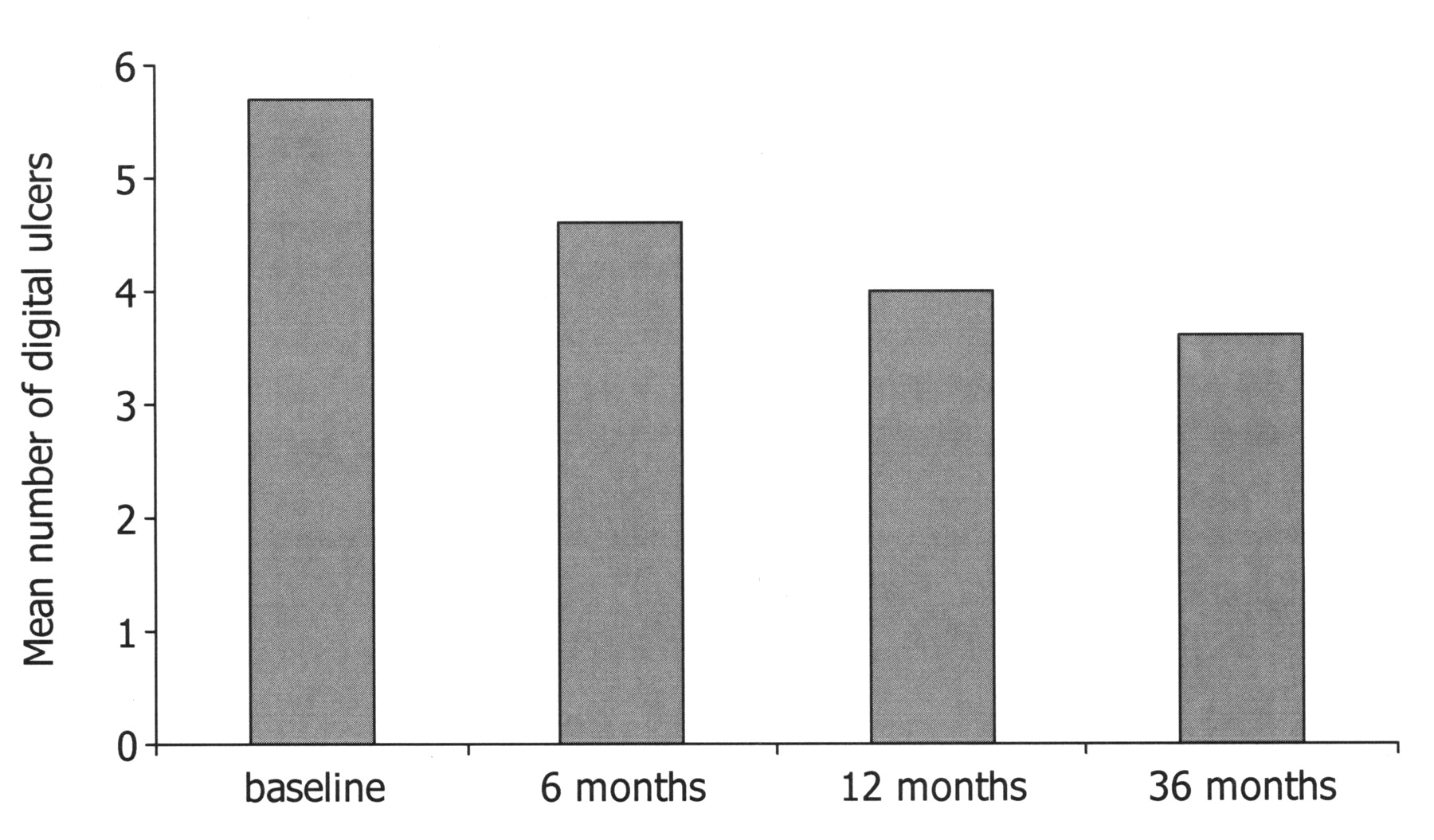
The mean number of DU per patient was reduced during the followup (6th mo and 12th mo) and at the end of the study (36th mo). The change was statistically significant (p < 0.001) for the 3 observation times (Figure 1). Healing of skin ulcers occurred in 17/26 patients (65%) after a median period of 25 weeks (range 8–26 wks). A clear improvement was noted in 4 patients (15%) and new ulcers developed in 5 (19%). Of interest is the fact that patients with PH had clinical improvement (by measuring 6 min walk time) and 3 of them had healed DU, while 2 presented clear improvement. Skin biopsy from the affected area showed a significant histological improvement (Figure 2A, 2B). Three patients discontinued the study (11.5%): 2 because they had elevated transaminase levels after 1 year of treatment, while 1 patient had reduction of hematocrit after 16 months of therapy.
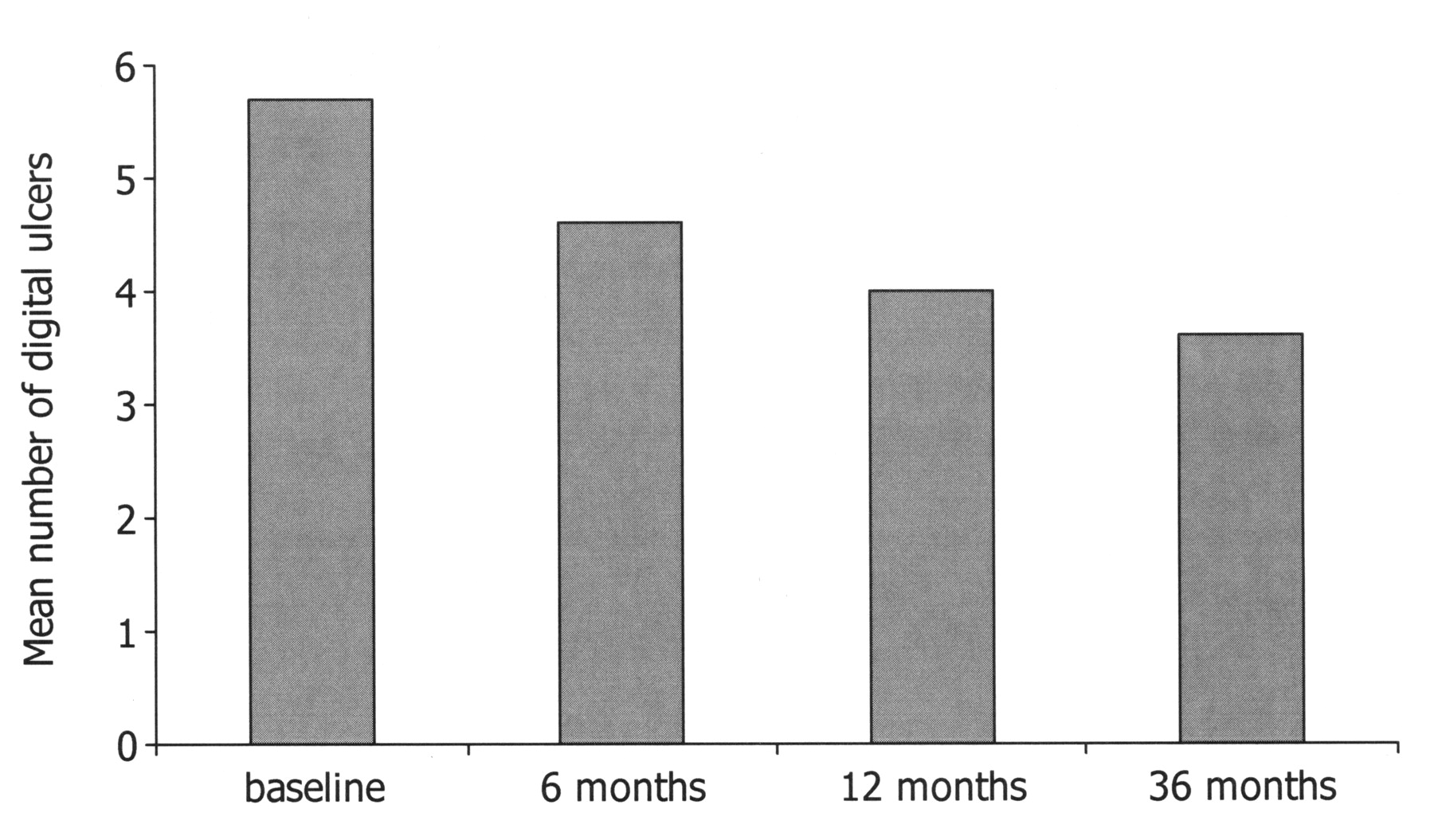
Mean number of digital ulcers (DU) per patient, at baseline and at specific times of followup. Mean number of DU was reduced during followup and at end of study with statistical significance (p < 0.001).
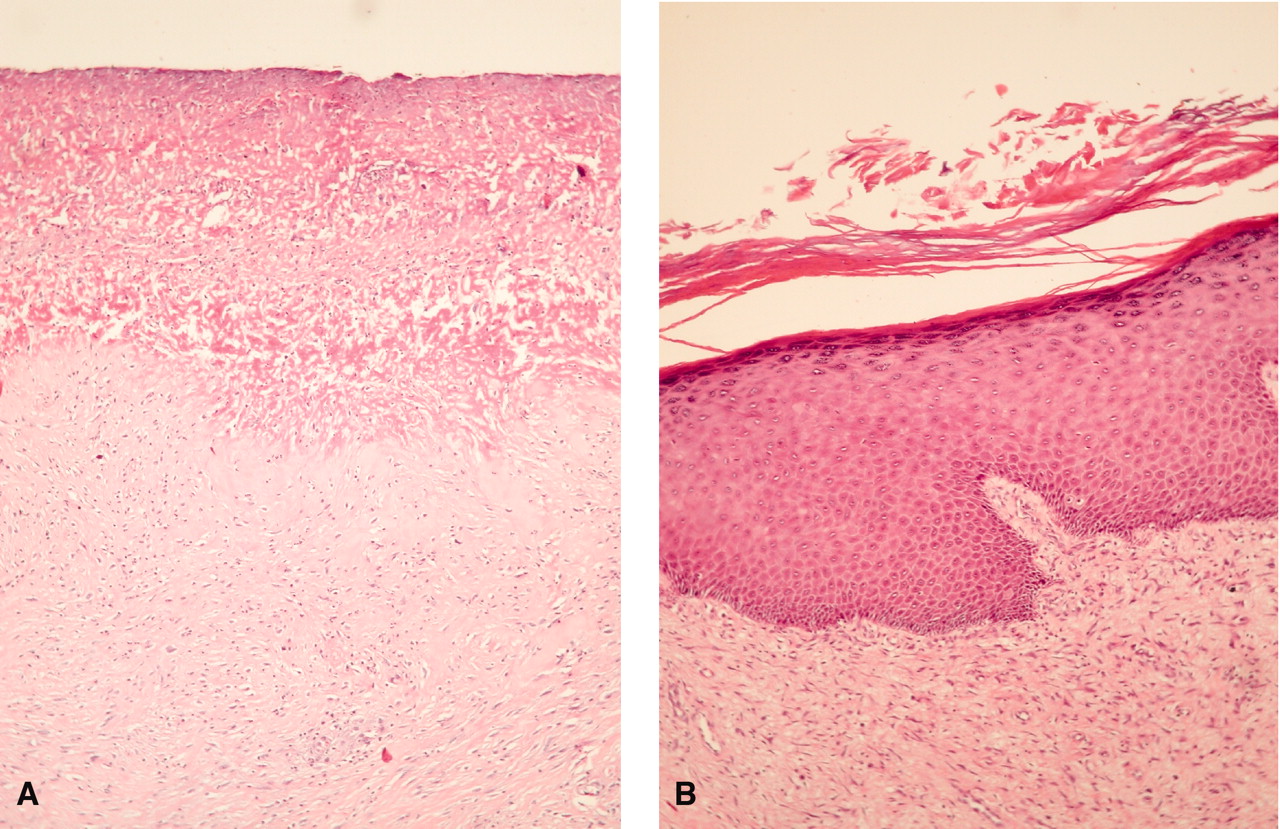
Skin biopsy before and after treatment with bosentan. (A) Before: the epidermis is ulcerated and surface coated by fibrinoid material with necrotic debris. The papillary dermis shows a dense infiltrate of neutrophils extending throughout the sclerosing reticular dermis. (B) After: the epidermis shows orthokeratosis, hypergranulosis, and extensive acanthosis. The dermis is sclerotic with increased number of fibrocytes. It shows dilated capillaries and dense infiltrate of lymphocytes, plasma cells, and occasional histiocytes.
DU are a common and debilitating problem for patients with SSc. Several agents are currently being used for the treatment and prevention of DU2,7–9. Recent double-blind studies, where the use of bosentan was compared to placebo, showed a decrease in the rate of new ulcer formation and improvement of the overall hand function score5. Other small series of patients showed the beneficial effects of bosentan on treating DU in SSc7. A recent open-label study of 15 patients with SSc and DU using bosentan for a median period of 24 months revealed that bosentan was safe and effective in these patients10. Ours is the longest prospective study that has evaluated the number of healed DU and new ulcer formation. We observed that healed ulcers occurred in 17 (65%) patients and a clear improvement in 4 more patients.
A limitation of our study is the small number of patients and its open-label design without a control group. We should emphasize, however, that all our patients were refractory to previous treatments and this is the only study in which DU improvement was demonstrated by skin biopsy.
Treatment with bosentan in patients with SSc has an acceptable toxicity profile and is effective in preventing and treating DU in a longterm fashion. However, other controlled studies with larger numbers of patients are needed to demonstrate the effectiveness and safety of bosentan in patients with SSc.








{kind=link}
{kind=link}