
Abstract
Objective. To investigate brain involvement in patients with systemic sclerosis (SSc).
Methods. Sixty-three patients with SSc fulfilling the American College of Rheumatology and/or Leroy and Medsger criteria were retrospectively studied, including 30 (47.6%) with limited cutaneous and 27 (42.9%) with diffuse cutaneous SSc. Forty-one patients underwent computed tomography (CT) scan and magnetic resonance imaging (MRI) of the brain, 11 patients only CT scan, and the remaining 11 patients only MRI. Cerebral vasculopathy on MRI and CT scan was defined as absent or mild (score < 1), moderate (1 ≤ score < 2), or severe (score ≥ 2) on a 4-point scale (0 to 3).
Results. Cerebral vasculopathy was identified on CT scan in 22 patients (moderate in 12 and severe in 10) and on MRI in 38 patients (moderate in 28 and severe in 10). Patients with severe cerebral vasculopathy seen on MRI were more likely to have pulmonary arterial hypertension (PAH; p = 0.003) and showed a tendency to have scleroderma renal crisis (SRC; p = 0.25, test for trend p = 0.097). A similar association was found between severe cerebral vasculopathy seen on CT scan and PAH (p = 0.026) or SRC (p = 0.04). After adjusting for age and hypertension, severe cerebral vasculopathy was still associated with increased risk of severe vascular manifestations [odds ratio (OR) 32, 95% confidence interval (CI) 3.45–297, p = 0.002 for CT scan; OR 26, 95% CI 1.71–394, p = 0.019 for MRI].
Conclusion. Severe cerebral vasculopathy is associated with severe vascular manifestations in SSc patients. SSc patients with severe vascular complications should undergo neuroradiological imaging assessment of brain involvement.
- CENTRAL NERVOUS SYSTEM
- SYSTEMIC SCLEROSIS
- COMPUTERIZED TOMOGRAPHY
- MAGNETIC RESONANCE IMAGING
- VASCULAR MANIFESTATIONS
Systemic sclerosis (SSc) is a rare multisystem disease characterized by vascular hyperreactivity, collagen deposition in the skin and internal organs, and autoimmunity with production of autoantibodies1,2. Vascular manifestations that include Raynaud’s phenomenon, digital ischemia, pulmonary arterial hypertension (PAH)3, and scleroderma renal crisis (SRC)4,5 are the consequence of endothelial injury and obliteration of the microvascular lumen6,7.
Since the first report of brain abnormalities in patients with SSc, dating from the pathological observations of Steven in 18988, signs and symptoms of brain involvement were infrequently reported in large clinical series of patients with SSc9. Thus, with brain involvement in these rare cases physicians should always look for another cause10, mainly renal or cardiopulmonary involvement11. Moreover, pathological examination detected cerebrovascular lesions no more frequently in patients with SSc than in an age-matched control group12.
In the last decade, few studies have provided evidence for specific brain involvement in SSc patients. Autopsy cases revealed calcifications of cerebral arteries, which suggests that SSc could induce primary cerebral vascular changes13. Pallidal and/or arterial calcifications involving the grey-matter nucleus of the brain were found in nearly one-third of SSc patients versus 10% in a control group on computed tomography (CT) scan of the brain13,14. More recently, white-matter lesions (WML) presenting as periventricular and/or parenchymal hypersignals seen on cerebral magnetic resonance imaging (MRI) were more frequently detected in SSc patients than in healthy controls15. However, the number of patients included in these series was small, and findings were not related to clinical manifestations of SSc.
We aimed to investigate brain involvement in a series of SSc patients by performing CT scan and/or MRI of the brain, to determine a possible relation between cerebral vasculopathy and usual vascular manifestations of SSc.
MATERIALS AND METHODS
Patient selection
SSc patients referred to the Internal Medicine Department of Avicenne Hospital from April 2000 to August 2003 and to the Internal Medicine Department of Cochin Hospital from September 2003 to January 2007 underwent CT scan and/or MRI of the brain. To be eligible for the study, SSc patients had to fulfill the American College of Rheumatology criteria16 and/or the Leroy criteria17 for SSc. Patients with SSc sine scleroderma had no detectable skin involvement18; limited cutaneous SSc (lcSSc) was defined by skin thickening in areas solely distal to the elbows and knees, and diffuse SSc (dSSc) was defined by the presence of skin thickening proximal, as well as distal, to the elbows and knees19.
Clinical, biological, and immunological assessment
Clinical characteristics recorded retrospectively included age at the time of diagnosis of SSc, age at the time of neuroradiological imaging; disease duration at the time of neuroradiological imaging; sex; ethnicity; Raynaud’s phenomenon; disease form; skin thickening assessed by the modified Rodnan skin score20; pitting scars; digital ulcers; digital infarcts; joint and/or muscle involvement; dyspnea (assessed by the New York Heart Association criteria21); heart involvement corresponding to conduction block or arrhythmia and/or cardiac insufficiency defined on a clinical and/or echocardiography basis with evidence of left ventricular systolic or diastolic dysfunction; and interstitial lung disease defined on high-resolution CT scan of the chest and showing one or more isolated ground-glass opacities, honeycombing, presence of ground-glass attenuation, and traction bronchiectasis and/or bronchiolectasis. Patients were evaluated with pulmonary function tests investigating forced vital capacity, total lung capacity, and diffusion capacity for carbon monoxide; restrictive syndrome defined by total lung capacity or a forced vital capacity < 80% of predicted values; PAH detected by echocardiography, with a tricuspid gradient of 30 mm Hg (i.e., an estimated systolic pulmonary arterial pressure ≥ 30 + 10 = 40 mm Hg, assuming a right atrial pressure of 10 mm Hg in all patients), and confirmed by right-heart catheterization when possible; SRC defined by rapidly progressive oliguric renal insufficiency with no other explanation and/or rapidly progressive hypertension during the course of SSc; hypertension and systolic and diastolic arterial pressure; esophagus involvement defined by dysphagia, heartburn, and regurgitation; bowel involvement defined by malabsorption, pseudoobstruction and/or bacterial overgrowth; neuropsychological involvement such as headache, depression, cognitive impairment, sensorimotor deficiency, seizure, and stroke; and diabetes mellitus.
Biological and immunological characteristics recorded were hemoglobin level; platelet count; C-reactive protein level; serum creatinine level; presence of schistocytes (> 1%); antinuclear antibodies (Ab); anticentromere Ab; anti-extractable nuclear antigen Ab, including anti-Scl70, anti-RNP, anti-SSA/Ro, anti-SSB/La, and anti-Pm-Scl Ab; antineutrophil cytoplasmic Ab; anticardiolipin Ab; rheumatoid factor; and cryoglobulin.
Neuroradiological assessment
Evaluation of neuroradiological involvement was retrospectively assessed by FC, who was blinded to the clinical and biological features of patients. Cerebral vasculopathy was assessed by MRI and CT scan of the brain. MR examinations were performed on different 1.5 T MR units, using a head coil (quadrature or multichannel). The MR protocol varied slightly between MR platforms; however, the T2 [3000 to 4500/95 to 140 ms (TR/TE)] and FLAIR [8800 to 10000/130 to 150/1880 to 2300 ms (TR/TE/TI)] sequences were obtained by rapid spin-echo techniques. The pre- and post-contrast T1-weighted spin-echo sequence used identical parameters (TE minimum, TR ranging from 450 to 650 ms). The diffusion-weighted sequence corresponded to a single echo-planar spin-echo sequence with a b = 0–1000 s/mm2. The isotropic diffusion images were calculated from 3 diffusion acquisitions with the diffusion gradients sequentially applied along each of the 3 orthogonal axes. All sequences comprised 20 to 24 axial sections, 5 to 6 mm thick, with 0.5 mm or no gap, field of view 24 × 24 cm. Brain CT scans covered the whole brain with axial contiguous sections with 3 mm slice thickness on the posteriori fossa and 5 to 6 mm above the cerebellum tentoria.
Indeed, cerebral vasculopathy is assessed in neuroradiological imaging by the presence of leukoaraiosis, which reflects the brain injury related to small arteries and capillary disease. MRI [fluid-attenuated inversion recovery (FLAIR) sequence or T2-weighted sequence if FLAIR was not available] was used to evaluate WML by the semiquantitative Fazekas scale, yielding 2 separate brain WML scores: (1) subcortical and deep lesions; and (2) periventricular lesions. Each variable was scored on a 4-point scale of increasing severity: 0, normal; 1, punctate; 2, coalescing (representing an intermediate step between punctate and confluent lesions); and 3, confluent. Periventricular lesions were scored as 0, normal; 1, pencil lines and/or caps; 2, smooth haloes; or 3, irregular. The mean of these 2 variables defined the leukoaraiosis score assessed on MRI, which reflects the severity of cerebral vasculopathy22. On CT scan, WML were categorized by extent and severity by use of the Blennow scale. Extent of WML was recorded on a 4-point scale: 0, no visible WML; 1, WML localized to the frontal and/or occipital periventricular regions of the lateral ventricles; 2, WML localized to the same regions as in 1 but spreading towards the centrum semiovale; or 3, extensive WML coalescing with the centrum semiovale (extensive WML that involve the centrum semiovale). Severity of WML was also graded on a 4-point scale: 0, absent; 1, mild; 2, moderate; or 3, severe. The mean of these 2 variables defined the leukoaraiosis score assessed on CT scan, which reflects the severity of cerebral vasculopathy23. Cerebral vasculopathy on MRI and CT scan was defined as absent or mild (score < 1), moderate (1 ≤ score < 2), or severe (score ≥ 2).
Pallidal and arterial calcifications were also assessed on CT scan without contrast injection. Pallidal calcifications were categorized as none, unilateral, or bilateral. Arterial calcifications were categorized by the number of involved arterial territories (right carotid siphon, left carotid siphon, vertebro-basilar system) as none, 1 territory, 2 territories, or 3 territories.
Statistical analysis
Data are presented as mean ± SD or median for continuous variables and percentage for qualitative variables. The Fisher’s exact test and the chi-square test for trend for ordered categories were used as appropriate to compare qualitative variables and the nonparametric Mann-Whitney test to compare continuous variables. P < 0.05 was considered significant. Multivariate logistic regressions were used to assess the association between cerebral vasculopathy seen on CT and/or MRI and severe vascular manifestations of SSc (i.e., PAH and SRC). Statistical analyses involved use of Stata SE 9.2 (Stata Corp., College Station, TX, USA).
RESULTS
Clinical, biological, and immunological characteristics of patients with SSc
Sixty-three patients with SSc were included in the study. Demographic, clinical, biological, and immunological characteristics of patients at the time of cerebral imaging are depicted in Table 1. Patients were mainly female (female/male ratio: 8/1) of white ethnicity (white/black ratio: 4.3/1). Median age at diagnosis of SSc and time of cerebral imaging was 46 ± 14 years (range 13–74 yrs) and 52 ± 12 years (range 17–77 yrs), respectively. Twenty-seven (42.8%) patients had diffuse cutaneous SSc.
Demographical, clinical, biological, and immunological features of 63 patients with systemic sclerosis (SSc).
Hypertension was present in 9 patients (14%), with median systolic and diastolic blood pressures of 120 mm Hg (range 80–220) and 80 mm Hg (range 60–120), respectively. Two patients had diabetes mellitus (3%). Median systolic pulmonary artery pressure was 31 mm Hg (range 19–64), and PAH was detected in 11 (17%) patients. Right-heart catheterization was performed in 4 of these 11 patients, which confirmed diagnosis of PAH in all 4. Eight of the patients with PAH had pulmonary fibrosis; none had left ventricular dysfunction as assessed by echocardiography (and by catheterization in 4 patients). PAH was treated with bosentan, epoprostenol, and intravenous iloprost in one patient each. Seven patients (11%) had a history of SRC; 4 of these had hypertension. No patient was undergoing dialysis at the time of neuroradiological imaging.
Immunological tests revealed the presence of antinuclear Ab in 53 patients (84%), antitopoisomerase 1 and anticentromere Ab in 13 each (21%), as well as anti-dsDNA (n = 5), anti-SSA/Ro (n = 3), antiribonucleoprotein (n = 5) and antiphospholipid (n = 4) Ab, and rheumatoid factor (n = 4).
Neuroradiological findings
Forty-one patients underwent CT scan and MRI of the brain; 11 had only CT scan and the remaining 11 only MRI.
CT scan findings (n = 52 patients) are detailed in Table 2, with analysis of cerebral vasculopathy and the presence of pallidal and arterial calcifications. Arterial calcifications mainly involved carotid siphons (right in 22 patients and left in 20 others) and the vertebrobasilar arterial system (intracranial vertebral artery and basilar trunk in 1 patient each).
CT scan and MRI findings for the brains of 52 patients with SSc. All values are expressed in n (%).
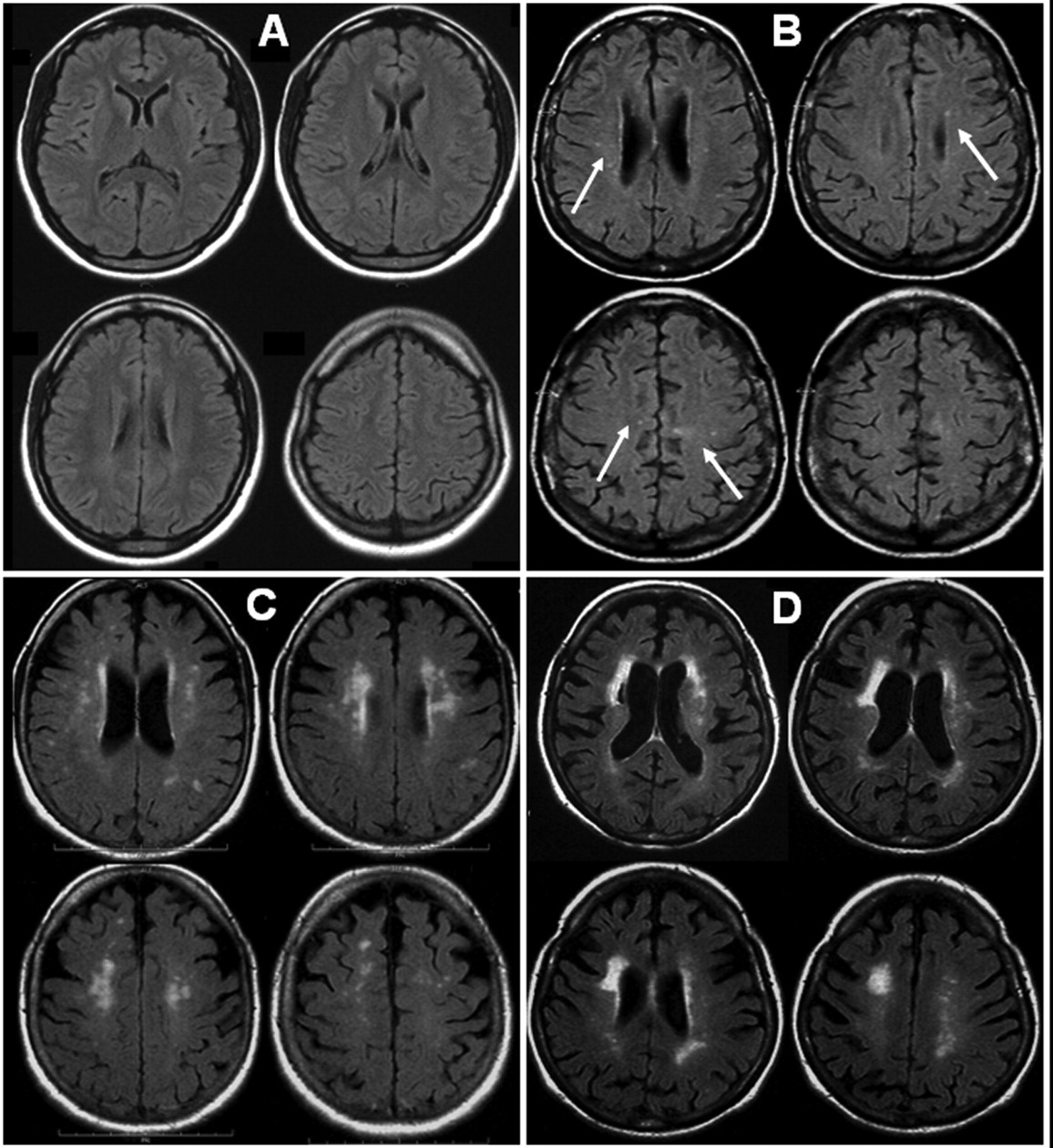
MRI findings (n = 52 patients) are detailed in Table 2. The MRI sequences performed were T1-weighted (n = 51), FLAIR (n = 48), T2-weighted (n = 37), diffusion (n = 18) and T1-weighted gadolinium enhanced (n = 45), as well as angio-MRI time-of-flight sequence of the polygon of Willis (n = 14). Cerebral vasculopathy was mild or absent in 14 patients (27%), moderate in 28 (54%), and severe in 10 (19%). Figure 1 shows MRI findings for the brains of patients without cerebral vasculopathy (A), with moderate cerebral vasculopathy (B), and with severe cerebral vasculopathy (C and D) as defined in Materials and Methods.

{kind=link}
Magnetic resonance imaging (MRI) using fluid attenuated inversion recovery (FLAIR) pulse sequence axial sections of the patient’s brain. Absence of cerebral vasculopathy (A), punctuate hyperintense white matter lesions (WML) classed as mild cerebral vasculopathy (B), and coalescing WML considered severe cerebral vasculopathy (C, D).
Ischemic sequelae were present in 5 patients (lacunar in 2, deep median cerebral artery in 1, junctional in 1, and superficial posterior in 1). The median age at the time of cerebral imaging of patients with ischemic sequelae was 63 years (range 41–77) and did not differ significantly from those without ischemic sequelae (55 yrs, range 17–73; p = 0.12). No recent ischemic lesion was found on diffusion sequence. No patient with severe cerebral vasculopathy on MRI had SSc sine scleroderma.
Among patients in whom CT scan and MRI were performed (n = 41), the time interval between the 2 examinations was less than one month. In these patients, among the 27 patients with absence or mild cerebral vasculopathy on CT scan, 13 had no or mild vasculopathy on MRI, 14 a moderate cerebral vasculopathy, and none a severe vasculopathy. Also, the kappa coefficient of agreement between the findings on CT scan and those on MRI was 0.50 (95% CI 0.29–0.70), indicating a poor concordance between the 2 techniques.
Association between cerebral vasculopathologic findings and vascular manifestations of SSc
We performed univariate analysis of patients with and without PAH, SRC, and digital ulcers/infarcts in terms of age, hypertension, diabetes mellitus, severe cerebral vasculopathy, and calcifications assessed on MRI and CT scan. Severe cerebral vasculopathy seen on MRI was associated with PAH (p = 0.003) and showed a tendency, although not significant, to be associated with SRC (p = 0.25, test for trend p = 0.097; Table 3). Severe cerebral vasculopathy seen on CT scan was associated with PAH (p = 0.026) and SRC (p = 0.04). Severe cerebral vasculopathy was not associated with the presence of digital ulcers/infarcts, nor were cerebral arterial calcifications associated with vascular manifestations of SSc. Finally, severe cerebral vasculopathy was strongly associated with severe vascular manifestations, defined as PAH and/or SRC, whether seen on CT scan (p < 0.0001) or MRI (p = 0.0009; Table 4). This relation still existed when analyses were restricted to nonhypertensive patients. In nonhypertensive patients, severe cerebral vasculopathy seen on MRI was associated with PAH (p = 0.004) and showed a tendency, although not significant, to be associated with SRC (p = 0.10, test for trend p = 0.10). Severe cerebral vasculopathy seen on CT scan was associated with PAH (p = 0.004) and SRC (p = 0.03). In contrast, severe cerebral vasculopathy was not associated with the presence of digital ulcers/infarcts, nor were cerebral arterial calcifications associated with vascular manifestations of SSc.
Univariate analysis of the association of factors related to cerebral vasculopathy seen on CT scan or MRI and severe vascular manifestations (pulmonary arterial hypertension, scleroderma renal crisis, and digital ulcer/infarcts).
Univariate analysis of the association between severity of cerebral vasculopathy and severe vascular manifestations.
After adjusting for age and hypertension, severe cerebral vasculopathy seen on CT or MRI was still associated with increased risk of severe vascular manifestations [odds ratio (OR) 32, 95% CI 3.45–297, p = 0.002 for CT scan; OR 26, 95% CI 1.71–394, p = 0.019 for MRI; Table 5].
Multivariate analysis of the association between severity of cerebral vasculopathy seen on CT scan and MRI and the presence of severe vascular manifestations (PAH and/or SRC) in patients with SSc. Cerebral vasculopathy on MRI and CT scan was defined as absent or mild (score < 1), moderate (1 ≤ score < 2), or severe (score ≥ 2).
DISCUSSION
In our study of CT scan and MRI of the brain in patients with SSc, we found severe cerebral vasculopathy associated with severe vascular manifestations, defined as PAH and/or SRC.
Recent studies provide evidence for specific vascular brain involvement in SSc patients, identified as calcifications of cerebral arteries on CT scan13,14 and WML on MRI15. Thus, Heron and colleagues reported in a series of 37 SSc patients and controls that intracerebral calcification was found in 12 patients (32.4%) and 7 controls (9.5%) (p = 0.006). In our study, pallidal calcifications were present in 12/52 patients (23%), which is lower than reported by Heron, et al14.
Sardanelli and colleagues reported in 2005 a series of 14 SSc patients and controls aged 24 to 74 years, and observed upon brain MRI that 170 white matter hyperintensities > 2 mm in diameter were counted in the patient group (range 0–75, mean 12.1, median 4.5), and only 13 in the control group (range 0–2, mean 0.9, median 1), a significant difference (p = 0.011). They did not describe further the extent of these white matter hyperintensities but provided a picture that could be interpreted as leukoaraiosis15. In that study, no statistically significant correlation between the number of hyperintensities and either patient age or disease duration was observed, but the number of patients tested was small.
Despite the absence of a control group, our findings agree with those of reports describing a particularly high proportion of SSc patients with moderate or severe cerebral vasculopathy. The sensitivity of CT scan is lower than that of MRI, and cerebral vasculopathy might have been underestimated in our subgroup of patients who only underwent CT scan24. Indeed, in the patients in which CT scan and MRI were performed (n = 41), MRI seems to be more sensitive to detect moderate cerebral vasculopathy than CT scan.
Moreover, the strong association between severe cerebral vasculopathy and the occurrence of severe vascular manifestations of SSc supports the specific brain involvement in SSc. This association has never been reported and could represent a particularly important breakthrough in the setting of SSc. Indeed, lesions of leukoaraiosis were shown to result from structural changes affecting cerebral arteries and arterioles and might be a consequence of vascular hyperreactivity. Thus, in addition to PAH and SRC, cerebral involvement could represent one of the features of vascular involvement in SSc, and patients presenting with involvement of one of these organs should be investigated for the presence of vascular brain involvement.
Patients included in our study had severe SSc. Thus, 42.9% of them had diffuse cutaneous SSc, which is a higher proportion than usually observed in the literature25, and the proportion of patients with PAH or SRC was higher in our study than that found in other studies of SSc patients. Indeed, the estimated prevalence of PAH is between 8%3 and 12%26, and that of SRC is lower than 10%, probably close to 5%5,27. The high proportion of patients with severe disease in our series is probably a consequence of the recruitment of patients in our French national reference center for SSc.
The clinical significance of leukoaraiosis has been extensively studied. However, the clinical relevance of WML identified on MRI remains controversial, particularly in elderly individuals, and white matter changes by themselves are considered to have doubtful clinical significance28. More recently, severe WML were reported as an independent risk factor for risk for stroke in atherosclerotic patients, and increased number of WML during followup might be associated with subsequent stroke in patients with an initially mild level of WML29. Thus, the assessment of white matter involvement might represent a valuable tool to evaluate the future risk of stroke30.
Alternatively, leukoaraiosis might represent an intermediate surrogate in the analysis of stroke rather than a true risk factor of stroke31. Moreover, a considerable number of clues support the hypothesis that leukoaraiosis may be the result of ischemic injury to the brain, through structural changes affecting the small intraparenchymal cerebral arteries and arterioles32.
In the setting of SSc, our findings open new insights into the therapeutic management of patients. Indeed, patients with cerebral vasculopathy seen on CT scan and/or MRI could represent a potential target population likely to benefit from secondary stroke prevention therapies if this finding is a predictor of stroke, which is associated with particularly high morbidity and mortality30. However, trials of therapy are needed to clearly determine the influence of such drugs on morbidity and mortality of SSc.
Of note, the presence of digital ulcers, a particularly frequent and disabling vascular complication of SSc, was not associated with neuroradiological features of cerebral vasculopathy. Since all vascular complications shared common pathogenic features (i.e., vascular hyperreactivity and obliteration of the microvascular lumen), explanations for this heterogeneous association among vascular complications with cerebral vasculopathy are unknown. However, PAH, SRC, and cerebral vasculopathy represent life-threatening vascular complications, whereas digital ulcers, which represent certainly one of the more frequent and disabling complications of SSc, are infrequently life-threatening.
Besides the potential risk of stroke in patients with SSc, WML could be associated with increased risk of cognitive impairment. In a recent systematic review of studies based on validated questionnaires or rating scales, the prevalence of depressive symptoms was consistently high among patients with SSc across studies33; the prevalence of symptoms of depression and anxiety were 20% to 50% and 15% to 64%, respectively34–42. In SSc, depressive symptoms are high, even compared with other patient groups with use of similar methods of assessment, and no studies have assessed the effects of the disease course of SSc or treatment on depressive symptoms33. Studies of associations between neuropsychological involvement and neuroradiological imaging are lacking, but could improve diagnostic and therapeutic management. Also of interest, the new imaging techniques such as functional MRI, positron emission tomography (PET), and single photon emission tomography (SPECT) could represent important tools in the early detection of these neuropsychological manifestations.
Limitations in the design of our study should be noted. Indeed, due to the retrospective design, the limited number of patients, and the absence of a control group, our findings should be interpreted with caution. In addition, the absence of evaluation of cognitive function is a limitation of the study. Future studies are needed to analyze the correlation between MRI findings and cognitive function in scleroderma patients.
We provide evidence that cerebral vasculopathy identified upon imaging of the brain by CT scan or MRI is associated with severe vascular manifestations defined as PAH and SRC in patients with SSc. We propose that SSc patients with severe vascular complications should undergo neuroradiological imaging assessment. MRI of the brain seems to be more sensitive than CT scan to detect moderate cerebral vasculopathy.
Footnotes
-
Supported by the Association des sclérodermiques de France. AB, LG, and LM are members of the Groupe Français de Recherche sur la Sclérodermie.
- Accepted for publication February 25, 2009.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.