

Abstract
Objective. To examine the relation between serum chemokine levels and patient responsiveness to infliximab, and the influence of infliximab administration on serum chemokine levels.
Methods. Serum levels of the chemokines CX3CL1, CXCL8, CCL3, and CXCL10 were quantified prior to (at baseline) and after 30 weeks of treatment with infliximab in 20 patients using enzyme-linked immunosorbent assays. Disease status was assessed using the Disease Activity Score (DAS28). The response to infliximab was classified according to the European League Against Rheumatism (EULAR) response criteria.
Results. By 30 weeks, infliximab produced a significant overall reduction in DAS28 among the 20 patients with RA, although only 12 achieved a good to moderate response based on EULAR response criteria. A significant reduction in CX3CL1 was seen in the responsive group, although infliximab treatment had no significant effect on the serum levels of the other 3 chemokines. Comparison of patients with lower (< 2000 pg/ml) and higher (≥ 2000 pg/ml) basal CX3CL1 levels revealed that DAS28, erythrocyte sedimentation rate, C-reactive protein, and CX3CL1 levels were all significantly diminished by infliximab in RA patients with lower basal CX3CL1 levels, but not in those with higher basal levels. In addition, cell-surface expression of CX3CR1 protein in peripheral blood CD8+CD3+ T cells and mRNA expression of CX3CR1 in lymphocytes were both significantly downregulated after infliximab treatment in the responsive group.
Conclusion. Our results suggest that the CX3CL1-CX3CR1 system in patients with active RA may be sensitive to anti-tumor necrosis factor-α therapy, and confirm that CX3CL1 plays a crucial role in the pathogenesis of RA.
Rheumatoid arthritis (RA) is a systemic autoimmune disease characterized by inflammation of the synovial joints, infiltration by blood-derived cells, and eventual destruction of cartilage and bone, as well as various extraarticular signs and symptoms1. The tumor necrosis factor-α (TNF-α) blocker infliximab is a chimeric IgG monoclonal antibody (mAb) that neutralizes both soluble and membrane-bound TNF in humans2. Several clinical trials have provided compelling evidence of the safety and clinical efficacy of infliximab for both the induction and maintenance of remission in RA. But although infliximab often induces rapid clinical improvement in patients with RA, 20%–40% of patients treated with infliximab show little or no clinical response3,4. Further, these patients may experience severe adverse effects, and the cost of infliximab therapy is very high. Consequently, identification of early predictors of the response to infliximab would likely have important clinical and economic benefits for the patients with RA.
Chemokines are a family of small proteins that regulate cell migration into sites of inflammation5. An important advance in our understanding of the development and progression of RA was the recognition that chemokines expressed in the synovium of RA joints are key mediators of cell migration into the joints, and are thus key contributors to the pathogenesis of RA synovitis6–10. In that context, our aim in this study was to examine the relation between serum chemokine levels and patient responsiveness to infliximab, as well as the effect of infliximab administration on serum chemokine levels.
MATERIALS AND METHODS
Patients
Twenty patients with active RA and who fulfilled the 1987 American College of Rheumatology (ACR) criteria11 were enrolled in our study between March 2005 and December 2007.All patients had active RA that, according to ACR guidelines12, failed to respond to treatment with methotrexate (MTX) or other disease modifying antirheumatic drugs (DMARD). No biological agents had been used in these patients, but glucocorticoids (< 10 mg/day of prednisolone) and nonsteroidal antiinflammatory drugs had to have been given at a stable dose for at least 4 weeks prior to enrollment and during the course of treatment in the study. Patients received intravenous infliximab at a dose of 3 mg/kg at baseline and at 2, 6, and 8-week intervals. Disease activity and its clinical improvement were assessed using Disease Activity Score (DAS28) [erythrocyte sedimentation rate (ESR) 4] with European League Against Rheumatism (EULAR) response criteria13,14. Patients with moderate to good responses to infliximab therapy were defined as the responsive group, while patients showing no response were defined as the unresponsive group. Serum and peripheral blood cells were collected immediately prior to (baseline) and 30 weeks after starting infliximab therapy. Serum rheumatoid factor (RF), matrix metalloproteinase (MMP-3), C-reactive protein (CRP) levels, and ESR were determined using a latex photometric immunoassay and the Westergren method, respectively. Anti-cyclic citrullinated protein antibody (anti-CCP Ab) was measured using commercial double ligand ELISA kit (Diastat Anti-CCP; MBL, Tokyo, Japan).
All experiments were carried out in accord with protocols approved by the Human Subjects Research Committee at our institution, and informed consent was obtained from all patients and volunteers.
Determination of serum chemokine levels
Serum levels of the chemokines CXCL8 [interleukin 8 (IL-8)], CXCL10 (interferon-inducible protein 10), CCL3 (macrophage inflammatory protein-1α), and CX3CL1 (fractalkine) were quantified using commercial ELISA kits according to the manufacturer’s instructions (R&D Systems, Minneapolis, MN, USA).
Flow cytometry
Flow cytometric analysis of CX3CR1 expression on peripheral blood mononuclear cells (PBMC) was carried out as described15. PBMC from heparinized venous blood collected from patients and healthy volunteers were labeled first with anti-CD3-FITC, anti-CD4-PE, anti-CD8-PE, anti-CD14 (monocyte)-FITC (all from BD PharMingen, San Diego, CA, USA), or rabbit anti-CX3CR1 Ab (ProSci Inc., Poway, CA, USA) and then with a secondary Ab (biotin-conjugated anti-rabbit IgG) and tertiary reagent (CyChrome-conjugated streptavidin; BD PharMingen). The fluorescence intensity and percentages of positive cells were measured on a 3-color FAC Scan flow cytometer (Becton Dickinson, Mountain View, CA, USA).
Isolation of total RNA and real-time polymerase chain reaction (PCR)
The monocyte fraction was isolated from PBMC using a monocyte isolation kit II (Miltenyi Biotec, Auburn, CA, USA), which included a cocktail of biotin-conjugated mAb against CD3, CD7, CD16, CD19, CD56, CD123, and glycophorin A. The purity of the CD14 expression was assessed with flow cytometry (> 95%). The remaining monocyte-depleted cell fraction was used as peripheral blood lymphocytes. Isolation of total cellular RNA from the lymphocyte and monocyte fractions and real-time PCR were all performed as described16. One-microgram samples of total RNA were reverse transcribed into cDNA using TaqMan RT reagents (Applied Biosystems, Foster City, CA, USA), after which real-time PCR was conducted using an ABI Prism® 7900 sequence detection system (Applied Biosystems). Detection of CX3CR1 and ribosomal RNA expression was accomplished using appropriate Assays-on-Demand™ primers and probes (Applied Biosystems). To make quantitative comparisons between different samples, a dilution series of pooled cDNA from unstimulated PBMC from healthy volunteers was used as internal standards for CX3CR1 and was loaded in each analysis. Maximum levels were assigned a value of 100 units.
Statistical analysis
Data were expressed as means ± standard error of the mean. The differences between groups were evaluated using the Mann-Whitney U-test. Followup data were evaluated using Wilcoxon’s test. The relationship between serum chemokine levels and the RA disease activity and indicated measures was evaluated using the Spearman rank correlation. Values of p < 0.05 were considered significant.
RESULTS
Kinetic study of serum chemokine levels in patients treated with infliximab
The patient characteristics are summarized in Table 1. At the start of therapy, the mean age of the patients was 55.4 years, disease duration was 5.9 years, and the baseline DAS28 was 5.79. Further, 19 patients were positive for anti-CCP Ab and RF. At baseline, there were no significant correlations between RA disease activity (DAS28) and RF, MMP-3, or anti-CCP Ab levels. There was also no significant correlation between the serum levels of any of the chemokines tested and either RA disease activity or serum measures including RF, MMP-3, and anti-CCP Ab levels (data not shown). Thirty weeks after the start of infliximab treatment, there was a significant overall reduction of RA disease activity (DAS28) from 5.79 ± 0.29 to 4.45 ± 0.27 (p < 0.05) among the patients. In addition, there was a significant reduction in serum CX3CL1 levels (baseline, 1926.7 ± 351.5 pg/ml vs 30 wks, 1533.3 ± 402.6 pg/ml; p < 0.05; Figure 1). Infliximab treatment had no significant effect on the serum levels of the other 3 chemokines tested (CXCL8, CXCL10, and CCL3), although levels of CXCL8 tended to be higher after infliximab treatment. Moreover, no significant reduction in serum levels of RF, MMP-3, and anti-CCP Ab levels were observed after 30 weeks of infliximab treatment (data not shown).

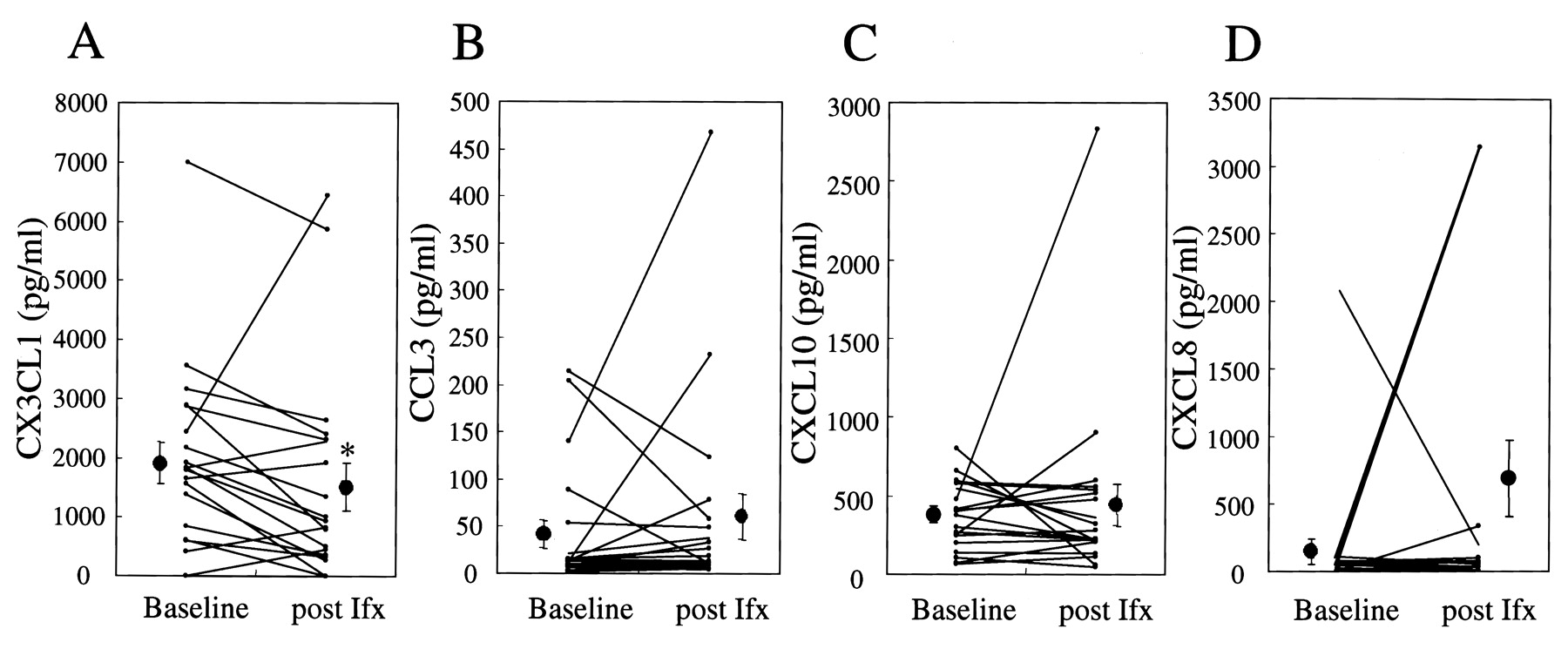
Changes in serum chemokine levels after infliximab administration. Paired serum samples from 20 patients with RA were collected at baseline and 30 wks after starting infliximab treatment. A: CX3CL1, B: CCL3, C: CXCL10, D: CXCL8. Each line represents an individual patient. Significant reduction of serum CX3CL1 was seen after infliximab treatment (*p< 0.05).
Patient characteristics.
We next analyzed the relation between changes in serum chemokine levels and clinical responses to infliximab therapy. At 30 weeks, 12 patients with RA showed a moderate to good response to infliximab based on EULAR response criteria, while 8 showed no clinical improvement. There were no significant differences between the responsive and unresponsive groups with respect to mean age, disease duration, doses of either MTX or prednisolone, serum anti-CCP Ab levels, or RA disease activity (DAS28; Table 1). Basal CX3CL1 and CXCL8 levels tended to be lower in the responsive group (CX3CL1, 1494.1 ± 266.3 pg/ml; CXCL8, 57.8 ± 9.9) than in the unresponsive group (CX3CL1, 2575.6 ± 755.7 pg/ml; CXCL8, 301.1 ± 254.2), but the difference was not significant. On the other hand, there was a significant reduction in serum CX3CL1 levels in the responsive group (1494.1 ± 266.3 vs 793.3 ± 219.8 pg/ml; p < 0.005), but not in the unresponsive group (Figure 2A). No significant changes were seen in the levels of CCL3, CXCL10, or CXCL8 in either group (Figures 2B, 2C, and 2D).

Serum chemokine levels between the responsive (n = 12) and unresponsive group (n = 8). Serum chemokines levels were measured at baseline and 30 wks after start of infliximab therapy. Clinical responses to infliximab were based on EULAR response criteria. A: CX3CL1, B: CCL3, C: CXCL10, D: CXCL8. Each line represents an individual patient. Significant reduction of serum CX3CL1 in the responsive group was seen after infliximab treatment (*p < 0.005).
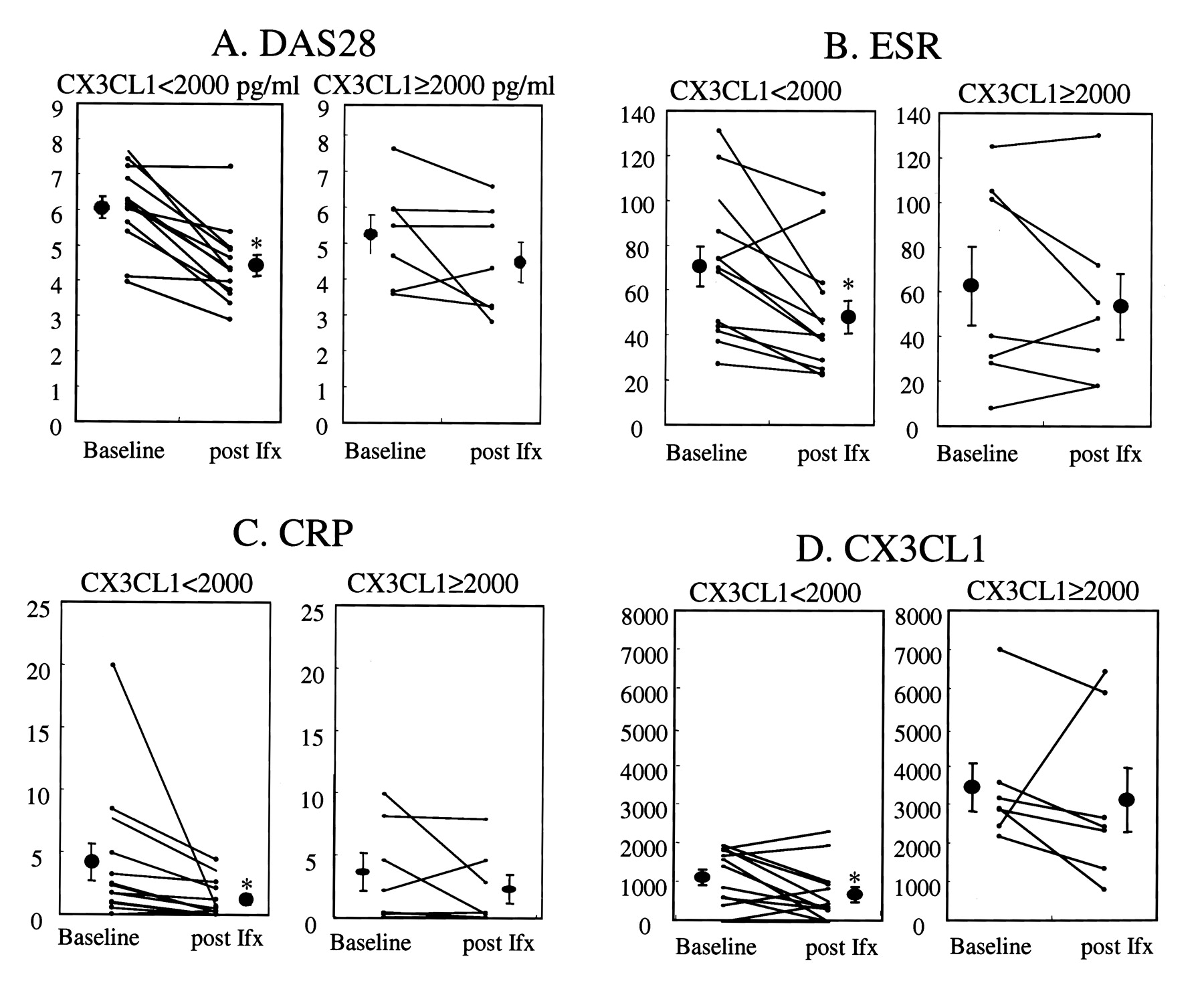
Because the results summarized above suggest that serum CX3CL1 levels may be related to RA disease activity and/or responsiveness of infliximab, we assessed the responsiveness of patients with RA to infliximab after dividing them into 2 groups based on whether their serum CX3CL1 levels were higher or lower than 2000 pg/ml. That criterion was selected because mean basal serum CX3CL1 level was 1926.7 ± 351.5 pg/ml for the entire study population. Comparison of patients with lower (< 2000 pg/ml, n = 13) and higher (≥ 2000 pg/ml, n = 7) basal CX3CL1 levels revealed no significant difference in DAS28, serum CRP levels, anti-CCP Ab levels, daily dosage of prednisolone, or weekly dosage of MTX (data not shown). DAS28, ESR, CRP, and CX3CL1 levels were all significantly reduced (DAS28 declined from 6.08 ± 0.32 to 4.43 ± 0.30, p < 0.0001; ESR, from 70.6 ± 8.9 to 48.2 ± 7.2, p < 0.01; CRP, from 4.2 ± 1.5 to 1.2 ± 0.4, p < 0.005; CX3CL1, from 1111.2 ± 200.7 to 682.7 ± 198.5 pg/ml, p < 0.05) in infliximab-treated RA patients with lower basal CX3CL1 levels (< 2000 pg/ml; Figure 3). By contrast, there were no significant reductions in DAS28, CRP, or CX3CL1 levels in patients with higher basal CX3CL1 levels (≥ 2000 pg/ml; Figure 3). In addition, there was no significant reduction in serum levels of RF, MMP-3, and anti-CCPAb levels after 30 weeks of infliximab treatment in patients with either higher or lower basal levels of CX3CL1 (data not shown).
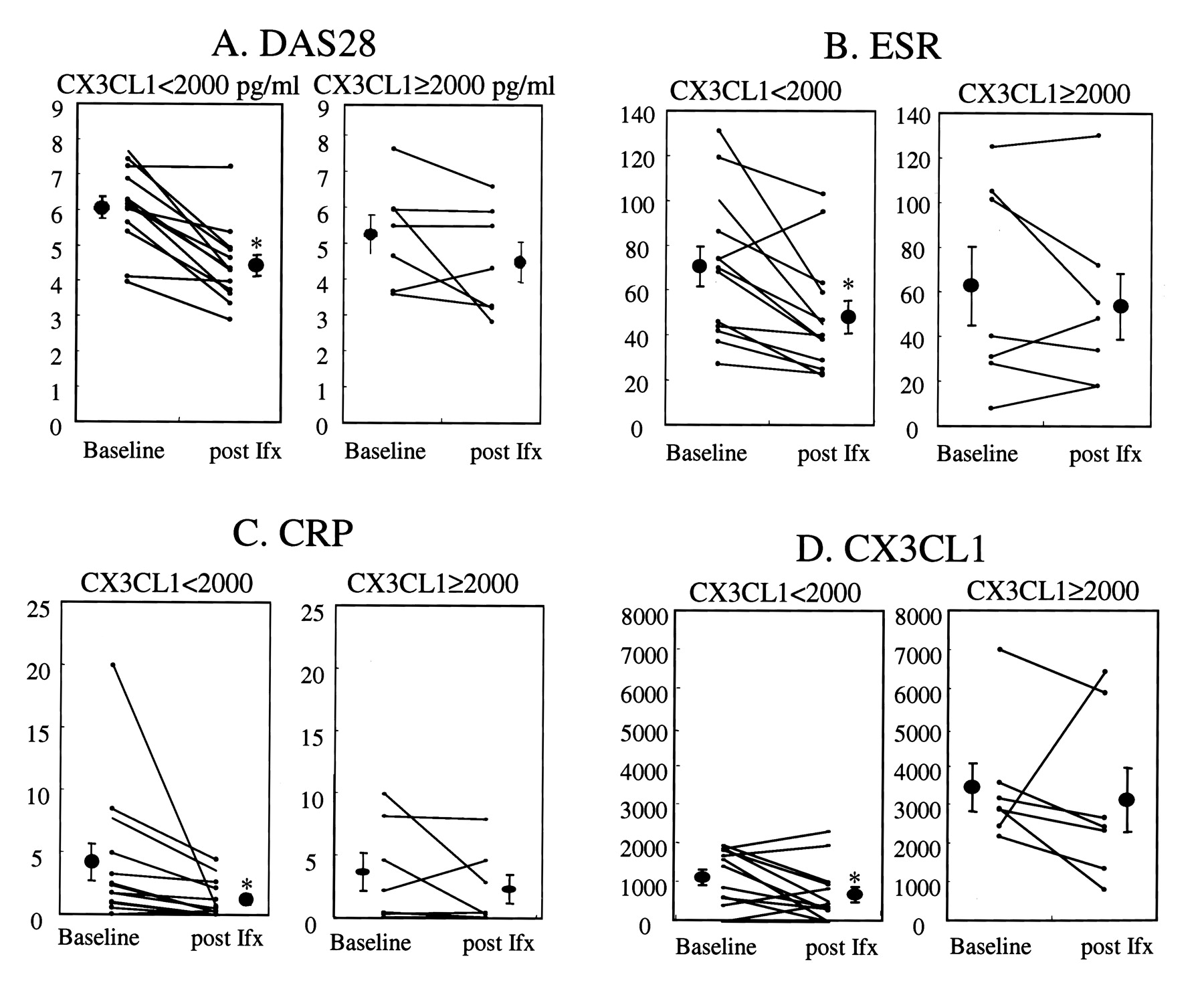
Effect of infliximab treatment on RA disease activity (DAS28), ESR, and serum CRP and CX3CL1 levels in RA patients with lower and higher basal CX3CL1 levels. Responsiveness to infliximab was statistically examined after dividing patients into 2 groups based on whether their basal CX3CL1 levels were higher or lower than 2000 pg /ml. DAS28 (A), ESR (B, mm/h), CRP (C, mg/dl), and CX3CL1 (D, pg/ml) levels were all significantly reduced (DAS28, p < 0.0001; ESR, p < 0.01; CRP, p < 0.005; CX3CL1, p < 0.05) in patients with lower basal CX3CL1 levels.
Increased cell-surface expression of CX3CR1 protein and CX3CR1 mRNA in patients with RA and their reduction by infliximab therapy
CX3CR1, a specific CX3CL1 receptor, is also crucially involved in the dysregulation of CX3CL1 expression under conditions of inflammation. To examine the phenotype of cells expressing CX3CR1 protein and mRNA, we used flow cytometry and real-time PCR to analyze their expression in peripheral blood-specific cell populations from 6 patients with RA randomly selected at the start of infliximab therapy and from 8 healthy controls. Mean fluorescence intensity (MFI) reflecting CX3CR1 expression was significantly (p < 0.05) more pronounced on CD8+CD3+ T cells from patients with active RA than on those from healthy controls (Figures 4A and 4B). No such difference was seen with CD4+CD3+ T cells or macrophages. Among the 6 patients with RA, 3 showed a moderate to good response 30 weeks after the start of infliximab therapy, while the other 3 showed little or no response. Notably, the MFI signals of CX3CR1 surface expression on CD8+CD3+ T cells were significantly reduced after infliximab treatment in the responsive group (Figure 4C), but not in the unresponsive group (Figure 4D). In contrast with CD8+CD3+ T cells, there was no significant alteration of CX3CR1 expression on either CD4+CD3+ T cells or macrophages (data not shown).

Cell-surface expression of CX3CR1 protein in PBMC from RA patients and its reduction after infliximab treatment. PBMC were obtained from 6 patients with RA and 8 healthy controls and labeled with anti-CD3+, anti-CD4+, anti-CD8+, anti-CD14+, and anti-CX3CR1 Ab. CX3CR1 expression on gated cells was then assayed by 3-color flow cytometry. A: Expression (mean fluorescence intensity; MFI) of CX3CR1 on CD8+CD3+ T cells from patients with active RA was significantly higher than in healthy controls. B: Representative dot plot graph of CX3CR1 expression on CD8+CD3+ T cells from patients and healthy controls. C and D: Expression of CX3CR1 on CD8+CD3+ T cells from 6 patients with RA [3 responsive (C) and 3 unresponsive (D) to infliximab therapy] randomly selected at the start of infliximab therapy. Data were expressed as MFI (units). Significant reductions in cell-surface CX3CR1 expression was seen in responsive group; p < 0.05 vs baseline.
Consistent with the reduced expression of CX3CR1 protein in those responsive to infliximab, basal expression of CX3CR1 mRNA tended to be lower in peripheral blood lymphocytes from responsive patients with RA (203.0 ± 22.7 units) than in those from the unresponsive group (489.7 ± 138.4 units), although the difference was not statistically insignificant. In addition, expression of CX3CR1 mRNA was significantly reduced after infliximab treatment in lymphocytes from responsive patients (n = 3), but not from unresponsive ones (Figure 5).
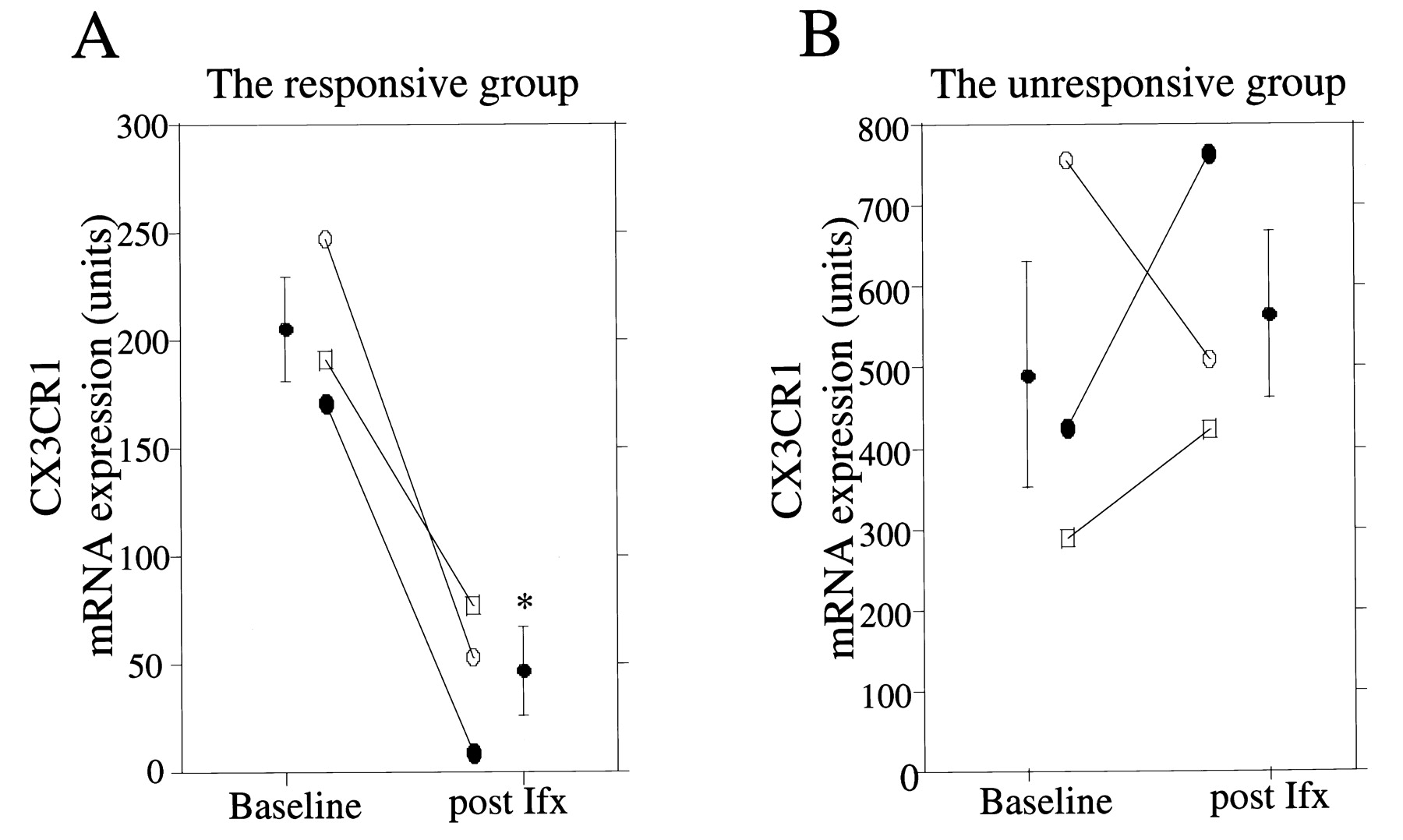
Expression of CX3CR1 mRNA in peripheral blood lymphocytes from patients with RA. Expression of CX3CR1 mRNA in peripheral blood lymphocytes from 6 patients [3 responsive (A) and 3 unresponsive (B) to infliximab therapy] randomly selected at the start of infliximab therapy. Data expressed in arbitrary units. Significant reductions in CX3CR1 mRNA were seen in responsive group; p < 0.05 vs baseline.
DISCUSSION
CX3CL1, CXCL8, CXCL10, and CCL3 all play crucial roles in the pathogenesis of RA6,9,10. We have shown that whereas serum levels of CXCL8, CXCL10, and CCL3 are unaffected by infliximab therapy, CX3CL1 levels decline in patients showing a clinical response to infliximab treatment. Moreover, patients with active RA who did not show a clinical response to infliximab showed higher basal CX3CL1 levels than those who did.
Expression of a variety of cytokines and chemokines, including IL-617,18, IL-1019, IL-1520, IL-1821, CXCL1622, and GROα (CXCL1)23 is reportedly blocked or diminished after infliximab therapy. Notably, all of these molecules are known to be induced in cells upon stimulation with TNF-α24, which suggests that inhibition by infliximab of TNF activity and its downstream cascade effectively suppresses production of these inflammatory cytokines and chemokines in patients with RA. Thus neutralization of endogenous TNF-α in patients with RA may underlie the clinical response to infliximab25.
The major cellular source of CX3CL1 in the periphery is the endothelium, and endothelium-derived CX3CL1 likely plays a pivotal role in such pathological conditions as vascular inflammation, glomerulonephritis, and systemic vasculitis26–29. In an earlier study, we showed that impaired endothelial cells within vasculitis lesions express CX3CL130. In addition, it was also recently shown that infliximab treatment reverses endothelial dysfunction in patients with RA31, and that otherwise elevated levels of soluble adhesion molecules (intercellular adhesion molecule-1, vascular cell adhesion molecule-1, and E-selectin) and vascular endothelial growth factor were significantly reduced by administration of infliximab to patients with active RA19,32,33. Thus infliximab may ameliorate endothelial cell activation, leading to downregulation of CX3CL1 expression.
Kageyama, et al reported that infliximab had no significant effect on serum CX3CL1 or CXCL10 levels in patients with RA22. We also found that infliximab had no significant effect on serum CXCL10 levels but, as discussed, we observed a significant reduction in CX3CL1 levels in some patients. Although the explanation for that difference in the response to infliximab is not clear, we did find that patients with basal serum CX3CL1 levels ≥ 2000 pg/ml were unresponsive to infliximab. Only when serum CX3CL1 levels were < 2000 pg/ml did infliximab have a beneficial effect in patients with active RA. Consistent with our findings are recent reports that RA disease activity is positively correlated with CX3CL1 levels in serum and synovial fluid, that expression of CX3CL1 is upregulated in inflamed synovial RA lesions, and that joint inflammation in an experimental arthritis model is reduced by neutralization of CX3CL130,34–37. TNF antagonists such as infliximab, etanercept, and adalimumab have only limited efficacy against pathological conditions related to systemic vasculitis38,39. We observed previously that serum CX3CL1 levels are significantly higher in patients with rheumatoid vasculitis or RA with extraarticular manifestations than in RA patients without vasculitis or other systemic manifestations30. We therefore suggest that patients with RA showing higher levels of CX3CL1 in this study may have latent vascular inflammation or vasculitis, resulting in a limited response against infliximab. These findings suggest that basal serum CX3CL1 levels may correlate with the responsiveness of patients with RA to infliximab therapy.
Expression of CX3CL1 and its specific receptor, CX3CR1, on CD8+ T lymphocytes was suppressed following TNF-α neutralization with infliximab in the responsive group. This may reflect diminished interaction between the endothelium and synovium, resulting in reduced infiltration of leukocytes (CD8+ T cells) into the rheumatoid synovium, which in turn likely reflects diminished CX3CL1/CX3-CR1-mediated chemotactic effects on monocytes, natural killer cells, and T lymphocytes. In addition, the CX3-CL1/CX3CR1 complex can also act as an adhesion molecule able to promote the firm adhesion of a subset of leukocytes to endothelium under conditions of physiological flow and of rheumatoid synovitis34,40–42.
It was recently shown that levels of IgM-RF antibodies are sometimes reduced following infliximab treatment, and that the progressive reduction of IgM-RF levels in patients treated with etanercept, another TNF antagonist, may have some prognostic importance43. Braun-Moscovici, et al showed that basal levels of anti-CCP antibody serve as a predictor of infliximab therapy18. In contrast, we could not detect any significant correlations between clinical response to infliximab therapy and serum levels of either RF or anti-CCP Ab. Although we did not examine the prognostic value of these antibodies in this study, further investigation of serum CX3CL1 in combination with other serum measures in larger numbers of patients should enable more precise prediction of the efficacy of anti-TNF therapy.
Our results suggest that the CX3CL1-CX3CR1 system in patients with active RA may be sensitive to anti-TNF-α therapy and confirm that CX3CL1 plays a crucial role in the pathogenesis of RA, although further investigations in a larger sample of RA patients with anti-TNF-α therapy are required to understand the clinical significance of CX3-CL1-CX3CR1. They also suggest that basal serum CX3CL1 levels correlate with the responsiveness of patients with RA to infliximab therapy.
Acknowledgments
We thank Mrs. Hiroko T. Takeuchi and Kyoko Nohtomi for their excellent help with the experiments.
Footnotes
-
Supported in part by a grant from the Ministry of Health and Welfare of Japan.
- Accepted for publication January 15, 2009.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}