

Abstract
Objective. Pulmonary endothelial dysfunction and increased reflection of pulmonary pressure waves have been reported in pulmonary arterial hypertension (PAH). However, the systemic vascular involvement is not fully understood. Our study focused on the systemic arterial stiffness and endothelial involvement in idiopathic and scleroderma associated PAH.
Methods. Peripheral arterial stiffness and endothelial function were evaluated in 38 patients with idiopathic (n = 28) and scleroderma associated (n = 10) PAH, and 21 control subjects (13 healthy; 8 with scleroderma and normal pulmonary pressure). All participants underwent clinical and cardiopulmonary evaluation. Arterial stiffness was measured through the fingertip tonometry derived augmentation index (AI), which is the boost increase in the late systolic pressure wave after the initial systolic shoulder. Endothelial function was measured by forearm blood flow dilatation response to brachial artery occlusion by a noninvasive plethysmograph (EndoPAT 2000), which is associated with nitric oxide-dependent vasodilatation and yields a peripheral arterial tone (PAT) ratio.
Results. Mean systolic pulmonary pressure was 70.5 ± 21.6 mm Hg (idiopathic-PAH) and 69.3 ± 20 mm Hg (scleroderma-PAH). AI was higher in scleroderma patients (10.5% ± 19.6% in healthy controls, 9.0% ± 21.5% in idiopathic-PAH, 20.1% ± 19.1% in scleroderma-PAH, and 24.4% ± 18.9% in scleroderma-controls; nonsignificant). PAT ratio was significantly lower (p < 0.05) than control values in idiopathic-PAH and scleroderma-PAH (PAT ratio: control 2.20 ± 0.25; idiopathic 1.84 ± 0.51; scleroderma 1.66 ± 0.66). AI was not correlated to endothelial dysfunction. There were no differences between the 2 PAH patient groups in age, body mass index, New York Heart Association classification, or 6-min walk test.
Conclusion. Our study shows a trend towards increased arterial stiffness in scleroderma (nonsignificant), and also peripheral endothelial dysfunction in idiopathic-PAH and in scleroderma-PAH. These findings suggest involvement of different vessels in scleroderma-PAH compared to idiopathic-PAH.
- PULMONARY ARTERIAL HYPERTENSION
- ARTERIAL STIFFNESS
- ENDOTHELIAL DYSFUNCTION
- AUGMENTATION INDEX
- SCLERODERMA
The histopathologic features of pulmonary arterial hypertension (PAH) include endothelial injury and proliferation1, which might affect endothelial function and vessel wall elasticity. Pulmonary endothelial dysfunction is apparently a significant component of the underlying mechanism of PAH1. PAH is characterized by impaired production of vasodilator mediators such as nitric oxide (NO) and prostacyclin along with overexpression of vasoconstrictors, such as endothelin-1 and thromboxane-A2 2–7. Pulmonary arterial compliance/stiffness is also dysregulated in PAH, with high reflection of systolic pulse waves in patients with idiopathic PAH (IPAH)8 and chronic thromboembolic pulmonary hypertension (CTEPH)9. The nature of the peripheral systemic vascular arterial stiffness and endothelial function in PAH is not understood.
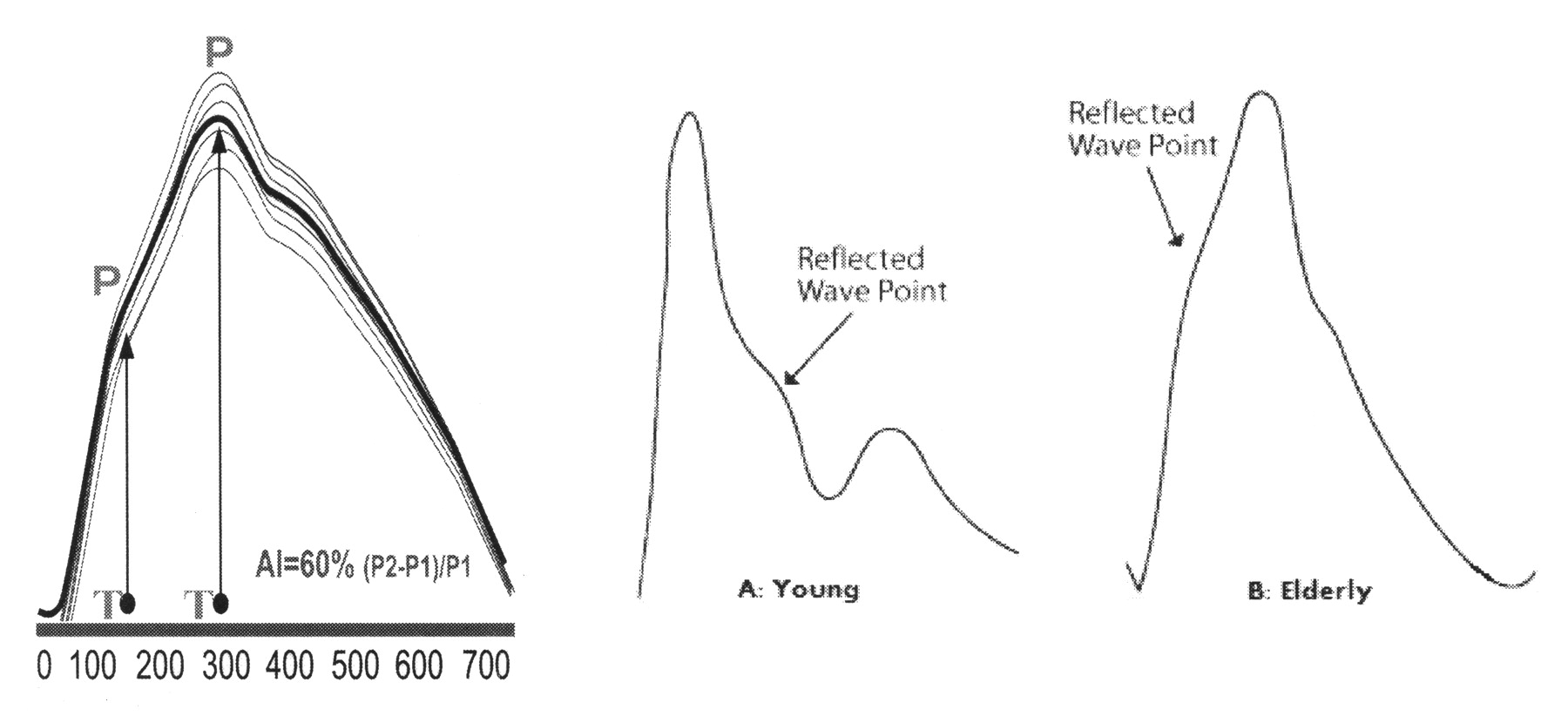
Arterial stiffness is determined by the force of cardiac contraction and vessel wall elasticity and compliance. Arterial stiffness is evaluated through the contribution of the reflected pressure wave to the systolic pressure signal impulse, named the augmentation index (AI). These reflections result in retrograde pressure waves, generated from sites of impedance mismatches, e.g., arterial branching10. The AI is defined as the difference between the first peak (caused by ventricular contraction) and the second peak (augmentation pressure) of the arterial waveform, expressed as a percentage of the pulse pressure (Figure 1)10–12. Normally, arterial elasticity converts pulsatile flow to a more constant flow, mainly in the proximal vessels13. Blood vessels with high compliance (i.e., low stiffness) experience only small systolic pressure increases with a relatively large increase in volume. Conversely, overly stiff central vessels cannot absorb more than a small fraction of each cardiac stroke volume without a substantial increase in pressure. Individuals with stiff central arteries (e.g., hypertensive or elderly persons)14,15 typically have relatively high systolic and pulse pressures and low diastolic pressure11, with increasing AI. Endothelial function testing reflects NO production in medium-small arteries. Nitric oxide is constitutionally expressed in normal endothelium and has vasodilatory, antiinflammatory, and antithrombotic properties. Peripheral endothelial function may be measured by a noninvasive plethysmograph (EndoPAT 2000; Itamar Medical, Caesarea, Israel), assessing post-occlusion brachial artery flow-mediated dilatation (FMD), which reflects endothelium-dependent reperfusion hyperemia16–22.

Augmentation index (AI) is the difference between the first (P1) and second (P2) peaks of the arterial waveform, expressed as a percentage of the pulse pressure [(P2 – P1)/P1]. A. Pulse wave of a young adult with low arterial stiffness (AI = −30%). B. An elderly adult: high arterial stiffness (AI = 30%).
In a previous study, we demonstrated peripheral endothelial dysfunction in patients with IPAH, scleroderma-PAH, and CTEPH and preserved endothelial function in PAH in patients with congenital heart disease associated PAH23.
The aim of our study was to investigate arterial stiffness in IPAH and scleroderma-PAH and its association with endothelial function. We hypothesized that patients with scleroderma will have increased peripheral arterial stiffness, compared to healthy controls and patients with IPAH.
MATERIALS AND METHODS
Study participants
Our study was prospective and cross-sectional. The study group included patients with IPAH or scleroderma associated PAH. The control groups consisted of scleroderma patients with normal pulmonary pressure and healthy controls. Medication was stable for 3 months prior to enrollment until the end of the study period. Exclusion criteria were diabetes, ischemic heart disease, cerebrovascular event, obstructive sleep apnea syndrome, renal failure, or systemic hypertension or concurrent medication with nitrates, alpha/beta blockers, and angiotensin-converting enzyme inhibitors. Obstructive sleep apnea was excluded due to a reversible endothelial dysfunction in this syndrome24.
Study protocol
All subjects underwent a full medical history, function class grading (New York Heart Association, NYHA), and physical examination. Laboratory assessment included pulmonary function tests, oxygen saturation (pulse oximetry), carbon monoxide diffusion capacity (DLCO), 6-min walk test, and transthoracic echocardiography. Twenty-four patients had undergone cardiac catheterization, and data on mean pulmonary pressure, cardiac index, and pulmonary vascular resistance were obtained from their records.
Pulse wave analysis was performed in the morning under stable conditions, after an overnight fast. Subjects were asked to refrain from smoking and from drinking alcohol or caffeinated drinks for 12 h. During testing, subjects were seated on a comfortable chair with both hands placed at the level of the heart. The Endo-PAT 2000 device (Itamar Medical) was used to obtain a beat-to-beat plethysmographic recording of the finger arterial pulse-wave amplitude (PWA). A pneumatic probe was placed on the index finger of each hand to record peripheral arterial tone (PAT). Following a 20-min equilibrium period (20°C constant temperature), baseline measurements were acquired over 5 min at rest. For AI measurement, the baseline signal from the rest period was used. AI was defined as the difference between the first (P1) and the second (P2) peaks of the arterial waveform, expressed as a percentage of the pulse pressure [(P2 – P1)/P1; Figure 1]. For endothelial dysfunction assessment, post-brachial artery occlusion wave was used. Occlusion was induced by inflating the cuff on the upper arm to 50 mm Hg above systolic pressure for 5 min and then releasing it to induce reactive (flow-mediated) hyperemia. The post-obstructive PWA was measured starting 90 seconds after cuff deflation, for 210 seconds. Endothelial function was calculated as the ratio between the average post-obstruction PWA and the average 3-minute baseline PWA, corrected for systemic changes and baseline signal amplitude. Both signals (AI and PAT) were analyzed with a computerized automated algorithm by the Endo-Pat 2000 system. Absolute endothelial dysfunction was defined as a PAT ratio of less than 1.6725,26. This FMD test has been used and compared with other methods16–22 in many previous studies17,18,25,26. Figure 2 presents examples of the normal and pathological (reactive hyperemia) pictures using the Endo-PAT 2000 device. The use of fingertip tonometry was validated previously and shown to be in close correlation with radial tonometry12,27,28.

EndoPAT 2000 signals. Normal (A) and abnormal (B) hyperemic response.
Our study was approved by the institutional review board of our center. All subjects signed an informed consent form to participate in the study.
Statistical analysis
Descriptive statistics were calculated for each group. Differences among the patient groups were analyzed by analysis of variance (ANOVA) and chi-squared test (contingency tables), and differences between patients and controls were analyzed by ANOVA. For post hoc analysis, the Scheffe test was used. A p value < 0.05 was considered significant. The Statistical Package for Social Sciences (SPSS Corp., version 15) was used for data handling and analysis.
RESULTS
Thirty-eight patients (28 IPAH; 10 scleroderma-PAH) and 21 control subjects (13 healthy; 8 scleroderma) participated in the study (Table 1). Mean pulmonary pressure was 70.5 ± 21.6 mm Hg in the IPAH group and 69.3 mm Hg in the scleroderma associated PAH and normal in controls (Table 1). Five patients were treated with epoprostenol, 7 with treprostenil, 7 with bosentan, 12 with other selective endothelin receptor blockers, 11 with sildenafil, and 7 with calcium channel blockers. Age, body mass index (BMI), and NYHA classification were similar in all patient groups. Comparison of the PAH patients with the control subjects yielded a statistically significant difference in NYHA class, baseline oxygen saturation, and DLCO. Where available, patients in the PAH groups had higher pulmonary artery pressures than the non-PAH scleroderma controls; none of the healthy controls had PA catherization data for comparison.
Clinical and epidemiologic characteristics of patients with pulmonary arterial hypertension (PAH) and controls.
Mean distance on the 6-min walk test was 399 ± 118 m in the IPAH group or 315 ± 77 m in the scleroderma-PAH (p = 0.044) group, although pulmonary hemodynamics, DLCO, and exercise desaturation were similar in both the PAH groups.
Arterial stiffness — augmentation index
AI was 10.5% ± 19.6% in healthy controls and 9.0% ± 21.5% in the IPAH group. In the scleroderma group, AI was twice as high: in the scleroderma-PAH group (20.1% ± 19.1%; nonsignificant) and 24.4 ± 18.9% in the scleroderma control group (nonsignificant vs healthy controls; Table 1, Figure 3). AI was positively correlated with age (Figure 4; r = 0.597; p = 0.001), but was not associated with the presence of PAH or other pulmonary or hemodynamic measurements.
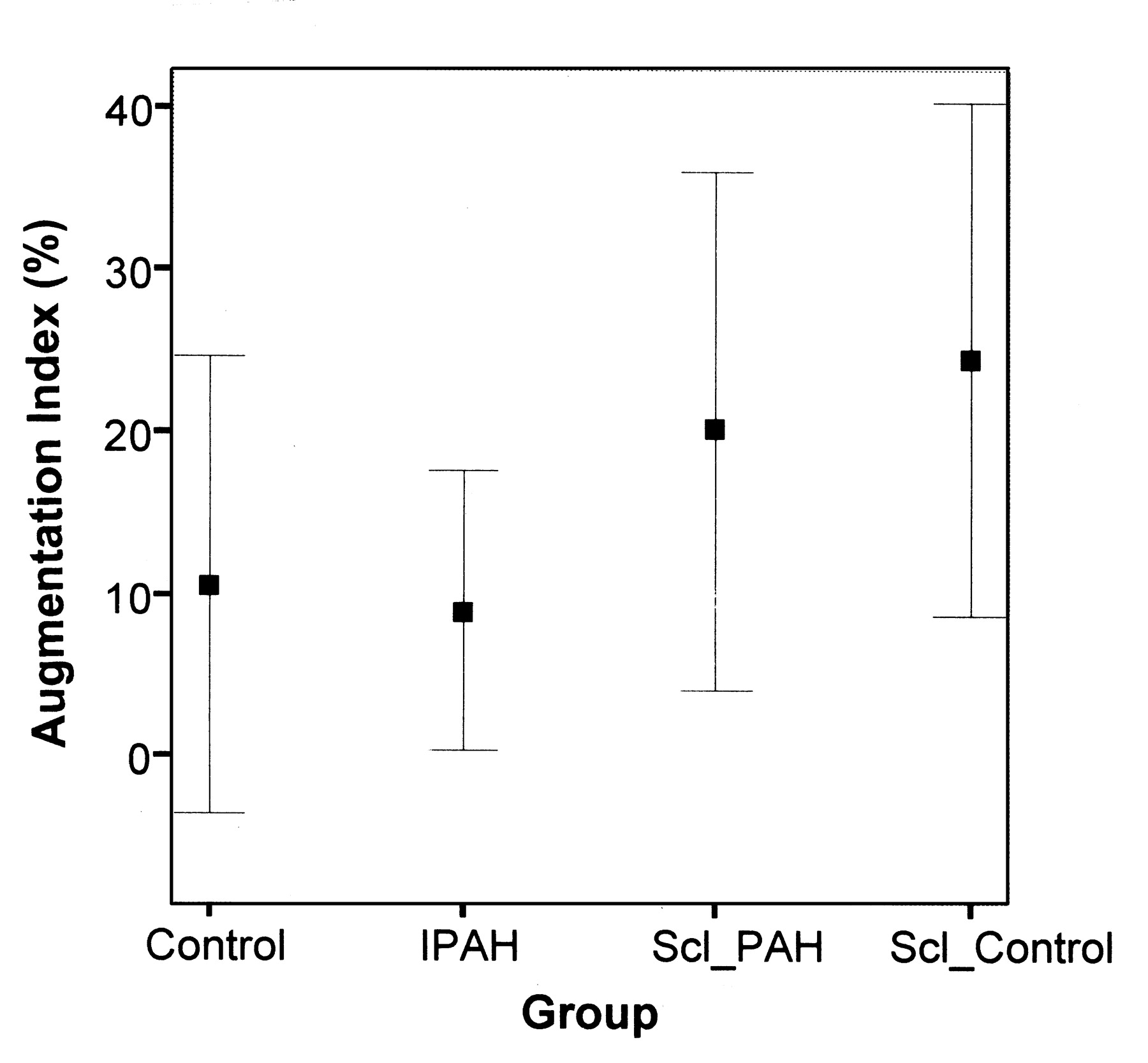
Augmentation index in all study groups (nonsignificant). Scl: scleroderma; IPAH: idiopathic pulmonary arterial hypertension.

Augmentation index and age in study subjects (r = 0.597; p = 0.001).
Brachial artery endothelial function
As we have reported previously, peripheral arterial endothelial function was significantly disturbed in IPAH (1.84 ± 0.51; p = 0.023) and in scleroderma-PAH (1.66 ± 0.66; p = 0.014) versus controls (PAT ratio: 2.20 ± 0.25). The scleroderma control group had similar PAT ratio (2.03 ± 0.38) as the healthy control group (Table 1)23. There was no correlation between AI and endothelial dysfunction.
Scleroderma with and without PAH
The patients with scleroderma and PAH were compared to age- and BMI-matched control subjects with scleroderma and normal pulmonary arterial pressure. The pulmonary hypertension group had worse clinical and cardiopulmonary measurements and had disturbed endothelial function (PAT ratio 1.66 ± 0.66 vs 2.20 ± 0.25; p = 0.014; Table 1). AI was similarly high in both groups (20.1% ± 19.1% and 24.4% ± 18.9%, vs 10.5% ± 19.6% in healthy controls; nonsignificant; Table 1, Figure 3).
DISCUSSION
In our study, 28 patients with IPAH, 10 with scleroderma-PAH, and 21 control subjects were assessed for arterial stiffness and endothelial dysfunction. Our analysis yielded 3 main findings: (1) peripheral arterial stiffness is normal in PAH and seems not to be correlated with PAH per se; (2) arterial stiffness has a tendency to be higher in patients with scleroderma, unrelated to the presence of PAH; (3) peripheral endothelial function is disturbed in IPAH and in scleroderma associated PAH.
Arterial stiffness is largely the result of progressive elastic fiber degeneration, mainly collagen and elastin29, but the endothelial30 and arterial wall smooth-muscle bulk and tone31 also play a role. Previous studies have shown that genetic polymorphisms of fibrillin 132, angiotensin II type 1 receptor33, and endothelin receptor gene are related to arterial stiffness. The normal pulmonary circulation exhibits very little wave reflection9, optimizing the right ventricular pulmonary artery coupling34. The pulmonary artery reflected wave is increased in conditions such as IPAH8,9 and CTEPH9. However, since increased reflected wave has been also reported in left heart failure35,36, one can speculate that the increased reflected wave seen in pulmonary circulation9,37 is secondary to the increased pulmonary arterial pressure, and is not a primary vascular wall abnormality per se. To our knowledge, our study is the first to report preserved systemic arterial stiffness in IPAH, as with normal age-dependent AI increase (15, Figure 4). In our cohort, the scleroderma group showed a trend towards increased AI, unrelated to the presence or absence of PAH (Table 1). This trend did not reach statistical significance — most probably due to the small sample size. An increased arterial stiffness in patients with scleroderma has been reported38–40. The increase in arterial stiffness has been shown to increase with the degree of endothelial inflammation soluble endothelial adhesion molecules, E-selectin, and soluble vascular cellular adhesion molecule-1, and is unrelated to endothelial dysfunction40.
Our previous findings23 of peripheral endothelial dysfunction in IPAH and scleroderma associated PAH and now the increased AI in scleroderma (Table 1) may indicate systemic endothelial involvement in scleroderma-PAH that is different from that seen in IPAH. Support for such systemic vascular involvement in PAH was provided by Hughes, et al41, who reported a significant reduction in brachial artery dilatation in patients with IPAH and their relatives, and in patients with systemic sclerosis with PAH. Additionally, Bull, et al42 observed a higher rate of circulating endothelial cells in patients with pulmonary hypertension, which was correlated with pulmonary pressure. Affected patients had higher values of CD36, a marker of microvascular origin, and of E-selectin, a marker of endothelial cell activation. The systemic involvement might be related primarily to the disease pathobiology, or mediated by a high activity of circulatory mediators in PAH such as proinflammatory cytokines43, alterations in metabolic pathways of serotonin44, prothrombotic abnormalities5,45,46, or hypoxia and sympathetic overactivity47.
AI was unrelated to endothelial dysfunction in our analysis. This finding is not surprising, since AI reflects arterial wall elasticity of large and medium size arteries13, while the hyperemic test assesses the endothelium for its ability to produce NO in the medium-small arteries22,40. Our findings are in agreement with Andersen, et al40, who failed to show association between AI and endothelial dysfunction in patients with scleroderma.
One confounding factor in our data was the use of PAH-specific drugs that may also modulate systemic endothelial function. To reduce variability, we measured endothelial dysfunction only in patients on stable regimens for 3 months prior to the study. Ethically, we could not stop the medication prior to the study. Nevertheless, the treatment regimen apparently had no effect on the reflected wave or the PAT signal (baseline or ratio; data not shown).
Our study demonstrates a trend towards increased arterial stiffness in patients with scleroderma, unrelated to their pulmonary pressure, and preserved arterial stiffness in those with IPAH with concomitant endothelial dysfunction. Arterial elasticity is unrelated to endothelial dysfunction per se. Since large vessels contribute to elasticity while medium and small vessels contribute to endothelial function, our study suggests that there is divergence in the location and nature of systemic vascular dysfunction between patients with scleroderma-PAH compared to those with IPAH.
Footnotes
- Accepted for publication December 30, 2008.








{kind=link}
{kind=link}
{kind=link}
{kind=link}