

To the Editor:
Early-onset gout is known to be often related to genetic factors. However, the molecular genetic issues are not understood for these patients.
In 2007, a 25-year-old Hong Kong Chinese man was referred for advice on his early-onset gout. The first of his many attacks was at age 18 years. A severe attack appeared at his right first metatarsophalangeal joint when he was 22 years old. His serum uric acid then was 600 μmol/l (10 mg/dl) and serum creatinine was 1.1 mg/l. His creatinine clearance was about 80 cc/min 3 years ago compared to 88 cc/min 10 years ago. He had 24-h uric acid excretion (using a low purine diet) at 5625 μmol/day (940 mg/day), indicating overproduction of uric acid.
The treatment of choice for gout with overproduction of uric acid is allopurinol, but the patient was worried about the safety of allopurinol because of his allergic history to other drugs and his father’s allergy to allopurinol. We suggested that the test of HLA-B*5801 might be helpful. The HLA-B*5801 allele was reported in one study to be present in all 51 (100%) Chinese patients with allopurinol-related severe cutaneous adverse reactions, but in only 20 (15%) of 135 allopurinol-tolerant patients (odds ratio 580.3)1. His HLA-B typing was *1302/*5401. Therefore, there was very little or no risk of allopurinol allergy for him. Thus, colchicine 0.5 mg daily plus allopurinol 100–300 mg daily was suggested to prevent gout attacks and renal stone formation.
To search for a cause of the overproduction, hypoxanthine-guanine phosphoribosyltransferase (HGPRT) and adenine phosphoribosyltransferase (APRT) activity were measured by high performance liquid chromatography2. HGPRT activity was in the normal range. To our surprise, his APRT activity was as low as 0.11 μmol/min per g hemoglobin (normal range 0.32–0.449). These data suggested that his gout might be related to partial deficiency of APRT, a very rare situation in a Chinese population. Allopurinol was also felt to be appropriate to treat this deficiency3,4. After 1 year and 2 months, he is taking allopurinol 250 mg daily and has been free of gout attack; his uric acid concentration is 5.7 mg/dl (338 μmol/l).
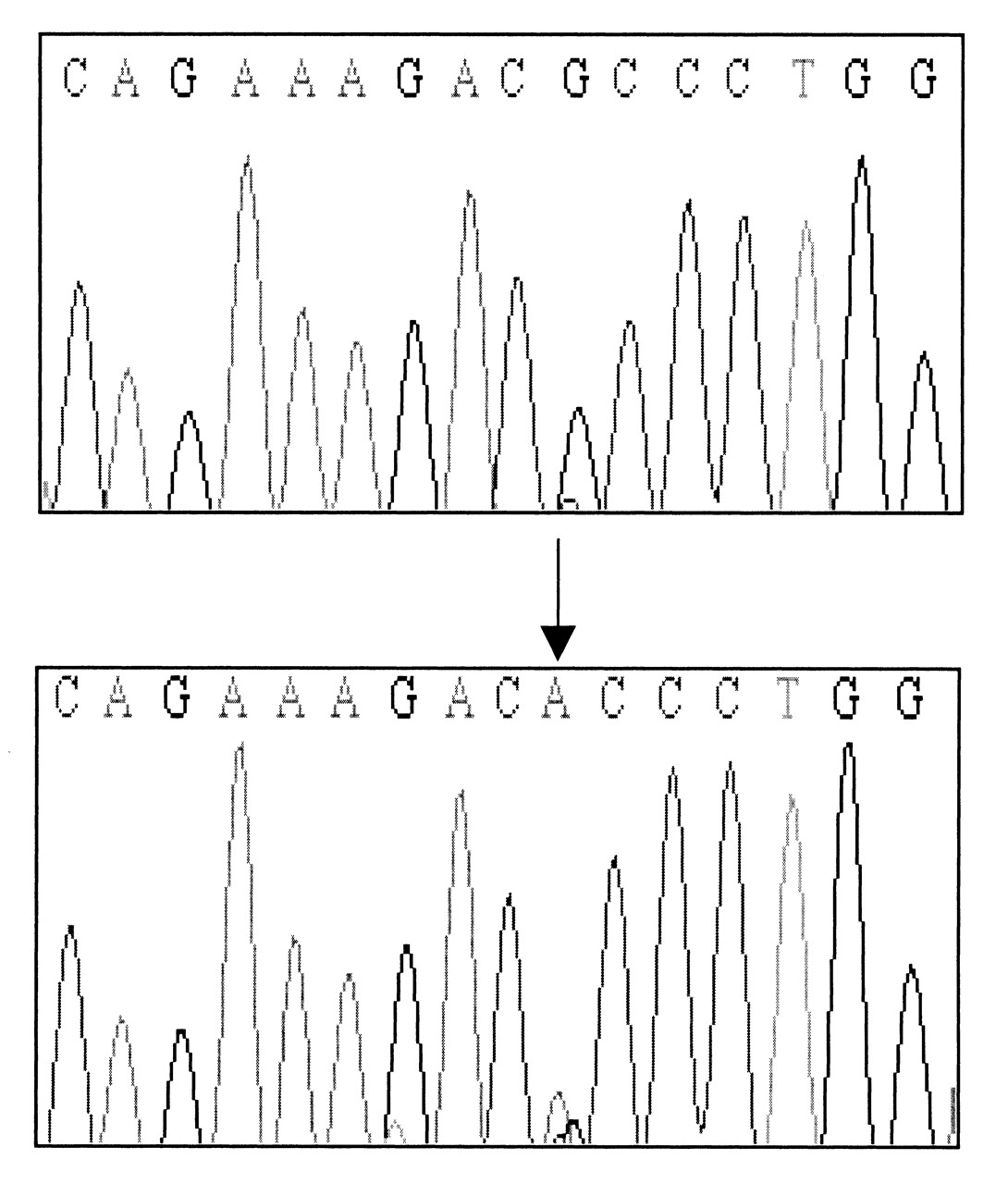
In further investigations, genomic DNA was extracted from buffy coats using a QIAmp DNA blood kit (Qiagen, Valencia, CA, USA). Polymerase chain reaction (PCR) was performed with the following primers; forward GCA TCG ACT ACA TCG CAG, and reverse CTG CAG GAG AGA GAA GAA G. PCR-DNA sequencing revealed a heterozygote mutation (G → A) at APRT base 346 (exon 4) resulting in substitution of alanine (GCC) by threonine (ACC) at codon 116 (Figure 1); thus, his APRT deficiency was caused by a novel APRT mutation.

PCR-DNA sequencing revealed a heterozygote mutation (G → A) at APRT base 346 (exon 4) resulting in substitution of alanine (GCC) by threonine (ACC) at codon 116.
APRT deficiency has been noted since 1968 and can be classified as complete deficiency (type I) or partial deficiency (type II)5. To date, 2 large population groups with APRT deficiency have been reported. In Iceland, 23 cases homozygous for type I APRT deficiency have been described4. Among these cases, 15 of whom had nephrolithiasis, 4 had mild to moderate renal insufficiency and one patient died of uremic complication4. In Japan, more than 120 cases with APRT deficiency have been reported6 and 78% were found to be type II. All type II patients carry at least one APRT*J allele with an ATG (methionine) to ACG (threonine) base substitution at amino aicd position 1366.
Evidently, our case represented a heterozygote mutation (G → A) at APRT base 346 (exon 4), resulting in alanine (GCC) to threonine (ACC) substitution at codon 116, which is different from the well known APRT*J in Japanese (Table 1). As well, the clinical presentation with early-onset gout in our case was also different from most reports describing presentation of nephrolithiasis or renal failure4,6.
Comparison of APRT mutations reported in Japanese, Icelandic, and Chinese populations.
Whether an APRT mutation is related to gout remains debatable. Kelley, et al reported the first APRT mutation in 19685. In 1974, Delbarre, et al found APRT deficiency in persons with gout, but they recognized that purine overproduction was not necessarily caused by the APRT deficiency7. In 1975, Emmerson, et al described a family with dominant inheritance of APRT deficiency. Although the female proband had gout, they could not confirm a relationship between APRT deficiency and gout8. To date, APRT deficiency has been regarded as a risk factor for gout by some Japanese investigators9; this has not been confirmed in other populations. In the future, a cohort study of cases with early onset-gout in Chinese or other populations may answer this question.
Footnotes
-
Supported by Chang Gung Memorial Hospital (CMRP 83014). We thank the patient and his family who agreed to publish this report to benefit patients with early-onset gout to get correct diagnosis and treatment. We thank Ming-Chi Yang for technical assistance.








{kind=link}