
Abstract
Objective. Delayed gadolinium-enhanced magnetic resonance imaging (MRI) of cartilage (dGEMRIC) is used to assess cartilage glycosaminoglycan distribution. Our aim was to determine the relationships between self-reported pain and disability, clinical variables, and serum leptin, and dGEMRIC indices in obese subjects with and without clinical knee osteoarthritis (OA).
Methods. Seventy-seven subjects were recruited from laparoscopic adjustable gastric banding or exercise and diet-weight loss programs. The dGEMRIC index was assessed on MRI according to established protocol. Regression analysis adjusted for age, sex, body mass index (BMI), and presence of clinical knee OA.
Results. Mean age and BMI were 51 ± 12.7 years and 39.6 ± 6.2 kg/m2. Twenty-three subjects (30%) had clinical knee OA (American College of Rheumatology criteria). The medial and lateral dGEMRIC indices were 538 ± 80 ms and 539 ± 86 ms. Age correlated negatively with medial (r = −0.40, p < 0.001) and lateral (r = −0.29, p = 0.012) dGEMRIC index. Subjects with clinical knee OA had significantly lower medial dGEMRIC index; however, no association was found for BMI. Varus alignment correlated with lower medial dGEMRIC index (r = −0.43, p < 0.006), while quadriceps strength correlated positively with lateral dGEMRIC index (r = 0.32, p = 0.008). There was also a negative correlation between serum leptin and lateral dGEMRIC index in women (r = −0.39, p = 0.035), with a trend in men (r = −0.52, p = 0.08). There were weak associations with physical disability, as self-reported on the WOMAC questionnaire.
Conclusion. In obese subjects, knee dGEMRIC index was associated with age, clinical knee OA, abnormal tibiofemoral alignment, and quadriceps strength. Longitudinal studies are required to assess the potential for improvement in dGEMRIC index with interventions such as strength training.
- DELAYED GADOLINIUM-ENHANCED
- MAGNETIC RESONANCE IMAGING
- LEPTIN
- MAGNETIC RESONANCE IMAGING OF CARTILAGE
- OBESITY
- OSTEOARTHRITIS
Osteoarthritis (OA), the most common form of arthritis, mainly affects the joint cartilage and is the leading cause of chronic disability among older people. Hyaline articular cartilage consists of a large extracellular matrix composed of water and proteoglygans entrapped within a collagenous framework. Proteoglygans are made up of glycosaminoglycans (GAG) attached to a backbone of hyaluronic acid1. Delayed gadolinium-enhanced magnetic resonance imaging of cartilage (dGEMRIC) is used to assess the relative distribution of GAG in cartilage noninvasively. This has been validated both in vitro and in vivo2. GAG are negatively charged due to abundant carboxyl and sulfate groups that are ionized at physiologic pH2. The technique utilizes a negatively charged contrast agent, gadopentate dimeglumine (Gd-DTPA2–; Magnevist; Berlex Laboratories, Wayne, NJ, USA), which when given time to penetrate cartilage tissue, distributes within cartilage matrix in an inverse relationship to the concentration of negatively charged GAG. Thus, the concentration of gadopentate dimeglumine will be relatively low in normal (GAG abundant) cartilage and relatively high in degraded cartilage (GAG loss)2. As gadopentate dimeglumine shortens the MRI parameter T1, the GAG content of articular cartilage can be estimated from T1 analysis within a specified cartilage volume after penetration of the contrast agent3. The mean T1(Gd) within a clinically relevant region of articular cartilage is referred to as the dGEMRIC index4, with low GAG content resulting in low dGEMRIC index and high GAG content yielding high dGEMRIC index5.
A high GAG content is essential for proper mechanical function of the cartilage and joints6, and significant in the maintenance of compressive stiffness7. In studies to date, the dGEMRIC index has been shown to be low in individuals with moderate to severe radiographic knee OA5, altered in knees with malalignment8, after cruciate ligament injury9,10, with exercise11,12, and in diseased knee compartments on arthroscopy13. A wide range of dGEMRIC indices have been noted in compartments with comparable radiographic severity grades, indicating perhaps differing rates of biochemical degeneration and thereby offering the potential to monitor the biochemical status of cartilage8. It also follows that dGEMRIC requires the presence of cartilage for meaningful assessment and has little utility in the presence of severe cartilage thinning. Consequently, it offers the potential to detect early changes in cartilage before radiographic change becomes evident. Clinically, this provides a window for early intervention and the opportunity to measure change.
Obesity represents a major public health problem, with the global burden of this condition rising at an alarming rate. The World Health Organisation estimates that more than 1 billion people are overweight and of these, 300 million are obese14. Large longitudinal studies have demonstrated that obesity is a significant risk factor for both the incidence and progression of tibiofemoral knee OA (both symptomatic and radiographic disease)14–16. Obese individuals also have higher cartilage defect severity and prevalence17. Leptin may represent the metabolic link between obesity and knee OA. Serum leptin, the product of the obese (ob) gene, is a cytokine-like pleiotropic hormone, involved in energy regulation at the level of the hypothalamus14. Leptin has been detected in synovial fluid samples obtained from patients with OA, levels correlating positively with body mass index (BMI)18. Recent work suggests that leptin is involved in OA development and affects cartilage metabolism directly as a proinflammatory cytokine, with consequent catabolic effects on cartilage19. The effects of leptin together with mechanical overload (due to activation of mechanoreceptors at the chondrocyte surface) may therefore act in concert contributing to the pathogenesis of OA20.
There is little information about the clinical associations of dGEMRIC indices in the knee. The aim of this cross-sectional analysis was to assess the dGEMRIC indices in an obese cohort, with and without clinical knee OA; and to determine the relationships between dGEMRIC index and self-reported pain and disability, objective physical measures, and serum leptin.
MATERIALS AND METHODS
Subjects
Our study was carried out in Northern Sydney between March 2006 and December 2007. Ethics approval for the study was obtained from the Northern Sydney Central Coast Area Health Service Human Research Ethics Committee and the University of Sydney, and informed consent was obtained from all study participants.
Patients were recruited from 2 avenues, and had voluntarily enrolled themselves in nonsurgical or surgical weight loss programs. All subjects were obese (BMI > 30), with most subjects being obesity grade 2 or higher, i.e., BMI > 35. The nonsurgical weight loss program, consisting of dietary modification and exercise, was conducted at the Metabolism and Obesity Services Clinic of Royal Prince Alfred Hospital in Sydney. In the surgical group, laparoscopic adjustable gastric banding was performed by 1 of 2 experienced surgeons at Royal North Shore Hospital in Sydney.
Between March 2006 and December 2007, all patients were screened during their initial visit at the respective centers and were offered the opportunity to participate in the longitudinal observational study. Clinical exclusion criteria: any inflammatory arthritis; psychiatric illness. MRI exclusion criteria: knee replacement surgery; weight > 150 kg; knee circumference > 52 cm; claustrophobia. dGEMRIC exclusion criteria: glomerular filtration rate (eGFR) < 60 mmol/l, pregnancy, or breast feeding. The American College of Rheumatology clinical classification criteria were used to define knee OA. This requires the presence of knee pain and at least 3 of the following: age > 50 years, morning stiffness < 30 min, crepitus, bony tenderness, bony enlargement, and no palpable warmth.
At the initial clinical assessment, demographic, clinical, and functional information was obtained. All subjects were asked to report on current (pain in the past month) and previous knee joint pain. Participants also underwent physical assessment by a rheumatologist, including knee range of motion; presence of patello-femoral crepitus; assessment of knee joint line tenderness, bony enlargement, and warmth; knee alignment22; and quadriceps muscle strength23. Knee range of motion was assessed as the difference in range between the knee in full flexion and full extension. Knee alignment was assessed as a continuous measure, with varus being negative, neutral 0, and valgus positive. Quadriceps strength was assessed as a continuous measure using a hand-held dynamometer, and the mean of 3 readings was obtained. Joint pain, stiffness, and physical function were assessed with the Western Ontario and McMaster Universities OA Index (WOMAC)24.
Serum leptin
A subset of subjects underwent fasting serum leptin measurement. This was limited by the availability of the assay at only 1 center. All leptin assays were conducted at the Rodney Shearman Endocrinology Laboratory at Royal Prince Alfred Hospital using uniform standard protocol; reference range for adult male (2.0–5.6 ng/ml) and female (3.7–11.1 ng/ml), respectively. This was assessed as a continuous variable.
Knee dGEMRIC assessment
Eligible subjects underwent MRI of the symptomatic knee at baseline prior to the start of their weight loss program. MRI was performed on a 3T scanner (Magnetom Trio; Siemens, Erlangen, Germany) with a transmit/receive knee extremity coil. Standard dGEMRIC protocol was applied with double dose (0.2 mM/kg) gadopentate dimeglumine (GdDTPA2–) administered 90 min prior to imaging9. Subjects were required to walk for 15 min after injection.
Two-dimensional single-slice dGEMRIC images were obtained in the medial and lateral sagittal planes with a fast spin-echo inversion recovery sequence with 5 inversion delays ranging from 50 to 2080 ms (TR 2200 ms; TE 14 ms). Slices were 3 mm thick with an in-plane resolution of 275 μm. T1Gd maps to calculate the dGEMRIC index were generated with a pixel-by-pixel 3-parameter T1 fit using Matlab software (The MathWorks, Natick, MA, USA). The dGEMRIC indices were calculated after manual segmentation for 4 regions of interest (ROI), 2 each from the medial and lateral sagittal sections, to yield the mean dGEMRIC index for an individual ROI, as well as averaged across-sagittal views to obtain the medial and lateral dGEMRIC index. The sagittal sections for dGEMRIC analysis were chosen from the center of each of the medial and lateral condyles. The dGEMRIC index was assessed for clinical associations with and without applying the BMI dose correction equation4. The dGEMRIC index corrected for BMI dose is referred to as the dGEMRIC index (BMI dose corrected) in the text. Full-thickness regions of interest in the sagittal plane consisted of weight-bearing femoral cartilage and all of the tibial cartilage. All images were read by a single trained observer (AA). Intraobserver reliability was measured using intraclass correlation coefficients (ICC) after repeat mapping 1 week apart for 10 subjects (ICC > 0.91 for each ROI). Our interobserver reliability for manual cartilage segmentation has been described25.
Statistical analysis
Spearman’s correlation analysis was used to analyze the association between the average dGEMRIC index in each ROI, medial and lateral dGEMRIC index against age, sex, BMI, and clinical knee OA. Linear regression was used to examine the associations between the collected clinical variables, self-report measures and serum leptin, and medial and lateral dGEMRIC indices. Multiple linear regression analysis adjusted for age, sex, BMI, and presence of clinical knee OA. A p value < 0.05 (2-tailed) or a 95% confidence interval not including the null point were considered significant. All statistical analysis was carried out using SPSS, standard version 14.0 (SPSS, Chicago, IL, USA).
RESULTS
A total of 288 potential subjects were screened from March 2006 to December 2007, 201 nonsurgical and 87 surgical patients. One hundred forty subjects agreed to participate and were recruited; 43 did not meet MRI/dGEMRIC criteria; 13 declined dGEMRIC scanning; 3 withdrew from the study prior to MRI scan; 4 were not able to attend MRI due to time commitments. A total of 77 subjects (79%) from the cohort therefore underwent dGEMRIC. In 1 subject, lateral sagittal views were not obtained. Severe cartilage thinning was identified in 9 ROI, thus yielding a total of 75 tibial ROI (medial sagittal), 72 femoral ROI (medial sagittal), 76 tibial ROI (lateral sagittal), and 74 femoral ROI (lateral sagittal) in the 77 subjects.
The main demographic characteristics of the study cohort are presented in Table 1. Thirty patients (39%) underwent laparoscopic gastric banding for weight loss, while the majority was involved in a formal dietary modification and exercise program. The mean WOMAC scores indicated a high level of joint pain and physical disability in this cohort.
Characteristics of the cohort (n = 77).
The dGEMRIC indices, with and without BMI dose correction, for each of the 4 ROI and averaged for each sagittal section are presented in Table 2. There was statistically significant negative correlation between age and dGEMRIC index regardless of BMI dose correction (medial dGEMRIC index, r = −0.40, p < 0.001; lateral dGEMRIC index, r = −0.29, p = 0.012). No significant sex differences were detected in the dGEMRIC index although women had slightly higher mean medial and lateral dGEMRIC indices. There was no correlation between BMI and dGEMRIC index in this obese cohort, with and without BMI dose correction. This observation remained unchanged when the groups with and without clinical knee OA were assessed separately. Subjects with clinical knee OA had lower medial dGEMRIC index (BMI dose corrected; 608 ± 76 without OA vs 562 ± 89 with OA; p = 0.032). This approached statistical significance for uncorrected medial dGEMRIC index (p = 0.058). There was no association between the presence of clinical knee OA and lateral dGEMRIC index. No correlations were observed between either pain or stiffness (WOMAC) and dGEMRIC indices; however, there were weak associations between self-reported disability (WOMAC) and low medial (r = −0.21, p = 0.07) and lateral (r = −0.20, p = 0.088) dGEMRIC index.
Baseline dGEMRIC index (ms), with and without BMI dose correction.
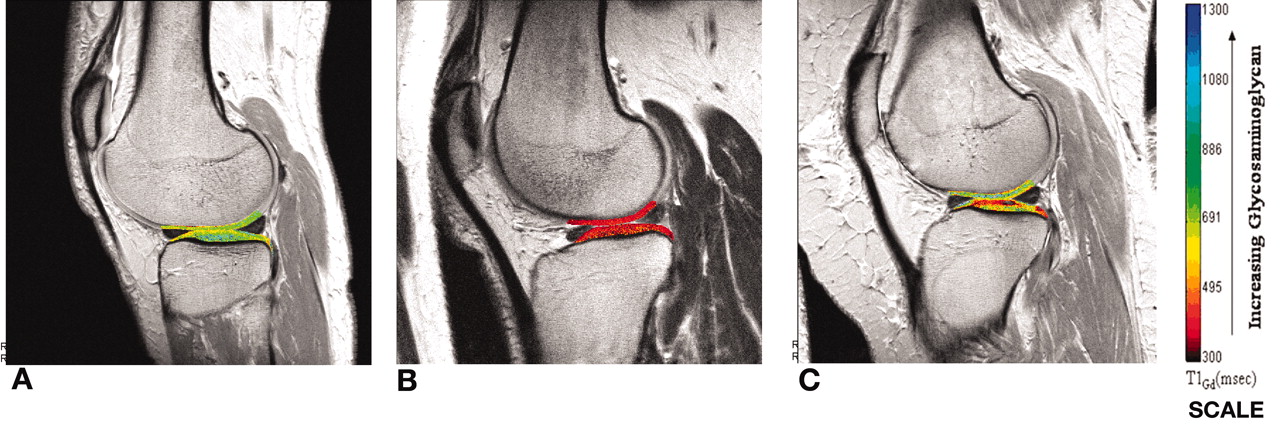
The multivariate model (age, sex, BMI, and clinical knee OA) accounted for 18% of the variance in the medial dGEMRIC index (p = 0.003, r2 = 0.18). More than half the cohort had focal areas of GAG loss as depicted in Figure 1C. These included subjects with and without clinical knee OA. Forty-one (53%) subjects had tibial cartilage focal GAG loss, and 42 (55%) had focal areas of GAG loss in the femoral cartilage. A majority, 60 subjects (78%), had focal areas of GAG loss in either the tibial or femoral cartilage. Femoral and not tibial focal GAG loss was significantly associated with the presence of clinical knee OA (p = 0.026). There was a trend to an association for any focal GAG loss and clinical knee OA (p = 0.065). Medial (tibial or femoral) focal GAG loss was significantly more common than lateral focal GAG loss (p = 0.005).

{kind=link}
The dGEMRIC index obtained after delayed gadolinium-enhanced MRI of cartilage. Examples of knees with (A) high global dGEMRIC index in cartilage; (B) low global dGEMRIC index in cartilage; and (C) focal areas of low uptake indicating selective GAG depletion.
Serum leptin
Forty-three subjects (56%) had serum leptin measurement with mean level 32.9 ± 13.0 and 56.8 ± 20.7 ng/ml in men and women, respectively, both well above the upper limit of reference ranges. BMI was positively associated with serum leptin (r = 0.31, p = 0.046). As the reference ranges for men and women were different, the groups were analyzed separately. In women, there was a significant negative correlation between serum leptin and lateral dGEMRIC index (r = −0.39, p = 0.035). A similar association was seen in men, approaching statistical significance (r = −0.52, p = 0.08). However, these associations did not remain significant in multivariate analysis with adjustment for age, sex, and clinical knee OA. No correlation was found between serum leptin and medial dGEMRIC index.
Physical measures
Varus alignment was significantly associated with low medial dGEMRIC index (with and without BMI dose correction; r = −0.43, p = 0.006). The association with low medial dGEMRIC index remained significant after adjustment for age, sex, and clinical knee OA (p = 0.043). No association was seen with valgus alignment and lateral dGEMRIC index. Greater quadriceps strength correlated positively with lateral dGEMRIC index (with and without BMI dose correction; r = 0.32, p = 0.006). These associations remained statistically significant in multivariate analysis with adjustment for age, sex, BMI, and clinical knee OA (p = 0.02; Table 3). There was no association between knee range of motion and medial dGEMRIC index. However, higher lateral dGEMRIC index was associated with increased knee range of motion (r = 0.31, p = 0.008). The multivariate model that included age, sex, BMI, knee OA, knee range of motion, varus knee alignment, and quadriceps strength accounted for 45% of the variance in medial dGEMRIC index (with BMI dose correction, r2 = 0.45, p = 0.005) and 44% of the variance in medial dGEMRIC index (r2 = 0.44, p = 0.008). In the lateral compartment, age, sex, BMI, knee OA, knee range of motion, and quadriceps strength accounted for 20% of the variance in dGEMRIC index (with BMI dose correction, r2 = 0.20, p = 0.018) (lateral dGEMRIC index, r2 = 0.17, p = 0.044).
Associations between dGEMRIC index and physical assessment variables*.
DISCUSSION
This cross-sectional study of 77 obese adults with and without symptomatic knee OA demonstrates important associations between clinical variables, physical measures, serum leptin, and dGEMRIC index in the knee (a surrogate measure of cartilage proteoglycan content).
To our knowledge, this is the first time a consistent negative correlation has been found between the dGEMRIC index and age. This association has not been observed in other studies utilizing dGEMRIC. This is in keeping with clinical expectation and also studies of other MRI measures. Ding, et al have shown that age is negatively associated with knee cartilage defect scores and prevalence in all compartments, knee cartilage thickness at all sites, and with patellar and not tibial cartilage volume26. The association between low dGEMRIC index and age is important clinically as it indicates that age affects not only cartilage and bone structure macroscopically but also cartilage ultrastructure, namely GAG content.
In our cohort, there was no correlation between BMI and dGEMRIC index with and without correction for BMI dose bias. This association was also not demonstrated when groups with and without clinical knee OA were analyzed separately. In a study by Tiderius, et al4, a significant negative correlation with corrected dGEMRIC index was only observed in the central weight-bearing femoral condyle in subjects with OA (contralateral knee) where radiographs demonstrated no joint space narrowing. They also found a trend for positive correlation between corrected dGEMRIC index and BMI in asymptomatic subjects4. A negative correlation between BMI and dGEMRIC index in subjects with OA has been reported4,8. However, in a study by Williams, et al8, the uncorrected dGEMRIC index was utilized. Hence, the associations between dGEMRIC index and BMI thus far have not been consistent. It is possible that the lack of association in our cohort may reflect a ceiling effect, as all our subjects were obese. While the range of BMI (30 to 51 kg/m2) would appear sufficient, the inverse association between BMI and dGEMRIC may have a threshold value, above which further increases in BMI are not resulting in even lower dGEMRIC indices.
Gd-DTPA2– is distributed solely in extracellular water (ECW) and is administered per kilogram body weight. As lean tissue has approximately twice the ECW content per unit weight as adipose tissue, it was postulated that differing body compositions may result in dosing bias with corresponding bias in the dGEMRIC index. The BMI dose correction equation was proposed by Tiderius, et al4 following an experiment measuring the plasma gadolinium concentration at various timepoints after Gd-DTPA2– administration in 24 individuals with varying BMI (range 21 to 47, most < 35). Interestingly, no differences in findings were detected when the authors reexamined other results applying the dose correction equation4. Similarly, we did not observe any major differences in the association with other clinical and physical measures, with or without correction for BMI dose. Hence, the BMI dose correction equation may not be necessary for future studies.
There was a high prevalence (30%) of clinical knee OA in this unselected obese cohort enrolled in weight loss programs, confirming the high risk of OA in this group. Subjects with clinical knee OA had lower medial dGEMRIC indices. As this was a heterogeneous obese cohort with and without knee pain and given the limitations of radiography, we chose to use a clinical definition of knee OA. This has previously not been used in MRI studies assessing knee dGEMRIC index, but we found similar correlations with clinical knee OA indicating that this definition may be a useful alternative in future trials. No sex differences were observed in relation to dGEMRIC index, in contrast to those seen in cartilage volume and thickness studies27.
Both global and focal areas of GAG depletion were observed in individuals with and without clinical knee OA; however, these focal areas were more likely to be present in subjects with clinical knee OA. Importantly, medial compartment (tibial or femoral) focal GAG loss was more common than for the lateral compartment. Interestingly, lateral dGEMRIC indices were higher overall compared to medial, although this did not reach statistical significance. Varying patterns of GAG loss have been observed, but no clear associations had been demonstrated5. It is not known whether this reflects a spectrum of OA severity or discrete pathological entities. It is also not known whether these areas of GAG depletion are reversible over time with measures such as weight loss or medication. Longitudinal studies are required to answer these pertinent questions and to determine whether these patterns of GAG loss have future clinical significance.
There were weak negative associations between serum leptin and lateral dGEMRIC index in both women and men. However, these associations did not remain after adjustment for potential confounders. Hence, the effects of leptin on dGEMRIC index may be mediated by factors such as BMI and age. The relationship between serum leptin and dGEMRIC index has not been examined previously. It is also possible that there may be a ceiling effect to the influence of high leptin levels on dGEMRIC index in this obese cohort, limiting the ability to detect associations in other compartments. In addition, only a subset of patients underwent serum leptin assessment. Nevertheless, the observations remained similar in both sexes. Larger observational studies may help clarify this association.
Varus aligned knees had lower medial dGEMRIC index. One study had shown only a trend for varus aligned knees to have lower dGEMRIC indices in the medial compartment8. We have demonstrated a definite statistical association for varus alignment after adjustment for confounders. The lack of association with the lateral compartment may be due to the reduced burden of lateral compartment disease. In addition, greater quadriceps strength was associated with a higher lateral dGEMRIC index. This was not observed for the medial compartment, but this may in part be due to the greater level of varus malalignment and burden of focal GAG loss affecting this compartment, offsetting potential gains from increased quadriceps strength in a sedentary obese cohort. The effects of quadriceps strength on dGEMRIC index have not been examined previously and require further evaluation. This finding perhaps offers the potential for intervention with strength training and requires assessment in future clinical studies. One study of middle-aged adults with previous partial medial meniscectomy, assessing only medial femoral dGEMRIC index, has demonstrated improvement after exercise intervention for 4 months12.
There were no associations between pain (WOMAC) and dGEMRIC index, but weak associations were detected between physical function (WOMAC) and dGEMRIC index. The lack of correlation with pain is not unexpected, as the correlation between the severity of structural damage and pain severity is poor, suggesting discordance between these measures. In addition, changes in GAG content probably reflect an earlier disease state in the manifestation of OA. Subchondral bone is recognized to be important in terms of pain and progression in OA29. Bone marrow edema/bone marrow lesions are typically visualized on fat-suppressed T2-weighted or STIR MRI images. These have been shown to be associated with knee pain in several studies29. With improving MRI technology it may be possible to combine these techniques to better assess pain and structure correlations, without a significant compromise in image acquisition time and patient comfort. The mechanism for the associations with physical function is not clear, but this may be mediated by the same pathway as joint range of motion.
Thus far, there have been few studies performing dGEMRIC assessment using a 3T MRI scanner. However, the mean values observed here, 500–700 ms, are similar to those reported in 2 other studies using 3T30,31, with population-based cohorts, mean BMI 26 to 27. A recent small study supported the dGEMRIC index as a clinically relevant measure of cartilage integrity, and suggested that a low index may be predictive of the development of knee OA3.
Ours is the first study to our knowledge to demonstrate associations of knee dGEMRIC index with clinical variables such as age and the presence of clinical knee OA, and physical measures such as quadriceps strength and tibiofemoral alignment. We also observed associations with serum leptin not previously described. This study provides valuable insight into the biochemical and biomechanical status of knee cartilage in a group vulnerable to developing and exhibiting knee OA. Longitudinal studies are required to assess the potential for change or improvement in dGEMRIC index with weight loss.
Acknowledgments
We thank Elisia Manson, Metabolism and Obesity Services, RPAH, and Sarah Fisher, NS Private Hospital for help accessing patient records; Peter Stanwell and Jeff McIntosh for performing the MR imaging; the Northern Clinical School, University of Sydney ARCHI (Advanced Research and Clinical High-field Imaging) for management of the 3T facility; Kris Tan, Endocrinology Laboratory, RPAH, for assistance with serum leptin levels; J.S. Chen, Rheumatology, RNSH, for statistical advice; Prof. Deborah Burstein, Department of Radiology, Beth Israel Deaconess Medical Center, Boston, Massachusetts, for her expert advice; and the study participants.
Footnotes
- Accepted for publication December 2, 2008.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.