
The symptoms of “fibromyalgia” are due to the interaction between referred pain and amplifying factors.
Given that Moldofsky and I described pain amplification related to measurable sleep disturbances1, we yield to no one in recognition of neural factors. Missing from Shleyfer, et al2 published in a recent issue of The Journal, from 2 commentaries in the current issue3,4, and from the long Wikipedia entry5 is any discussion of referred pain and of tender sites as markers of referred pain. These help identify the underlying somatic pathology, and therefore the necessary treatment and research strategies. Labeling alone doesn’t help; for a full diagnosis, definition of underlying problems and appropriate treatment strategies are required.
But there need be no talk of “war” among friends and colleagues (everybody loses wars). Disagreement should be the beginning of creative discussion.
The scientific study of referred pain began with the work of J.H. Kellgren6, with whom I had the privilege of working. I quote from a letter I received from him dated May 28, 1999, about 2 years before his death: “...When I started the experimental pain studies in 1936, it was believed that pain was accurately localized in all somatic structures and that only viscera gave referred pain through some special reflex. Our work at that time showed this to be false and led to a clinical method for ascertaining the anatomical source of all pains. This had a big impact on clinical diagnosis in medicine and surgery as well as rheumatology but has recently lost its interest since all the scanners and other machines have taken over....”
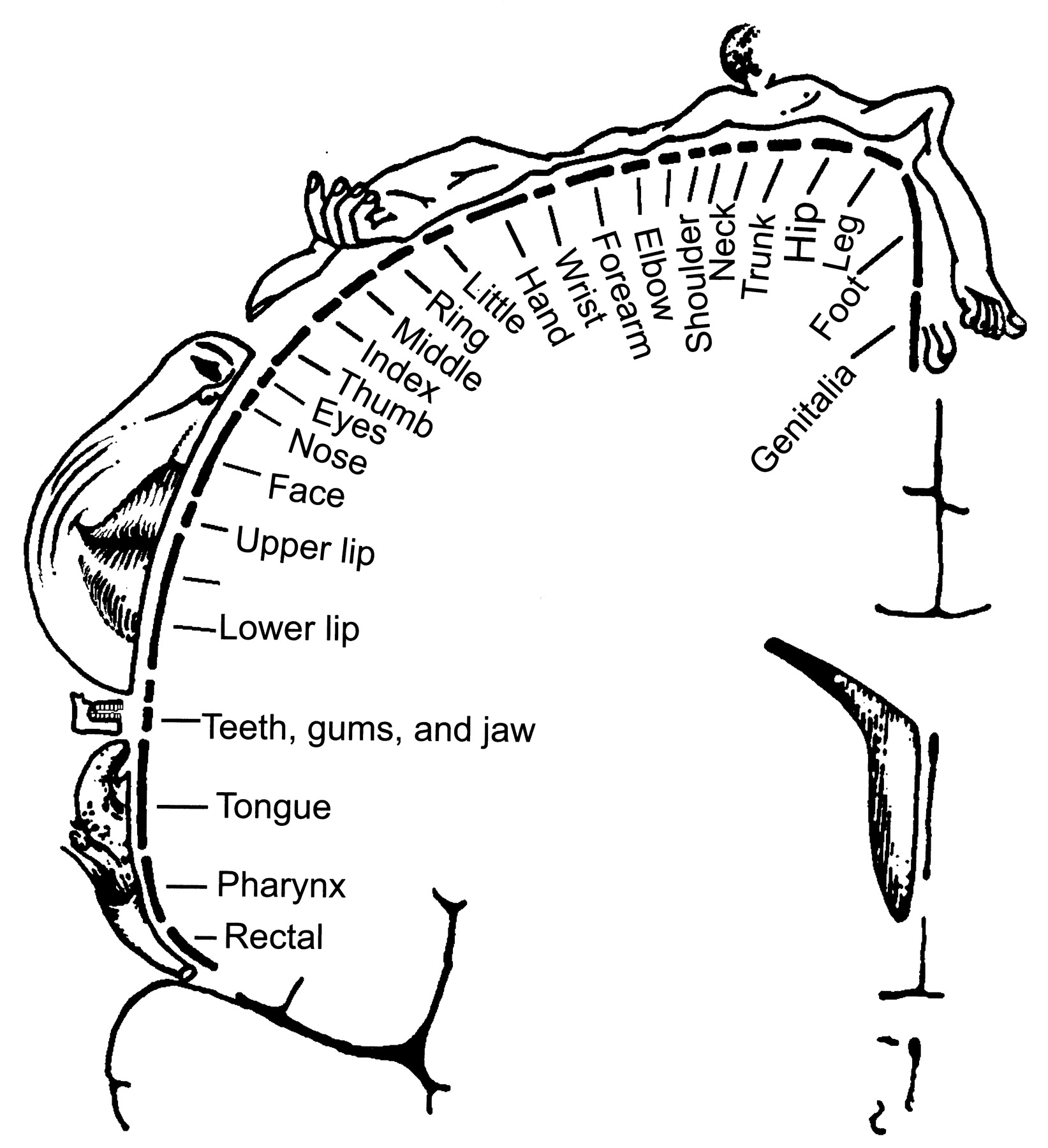
With great respect, I submit he overstated his case. When I trained, the work of Thomas Lewis and Kellgren was very fresh. We recognized certain features of referred pain, but there was no easy way to trace an origin in deep structures. Structured questionnaires cannot differentiate among possibilities. The reason for the difficulty is clear, when we reexamine another, independent gift from the 1930s, the sensory homunculus described by Penfield and Rasmussen7,8 (Figure 1).
{kind=link}
The human sensory cortex. Most deep structures, including lower cervical and lower lumbar vertebrae, are not represented. Pain referred from these often gives rise to medically unexplained symptoms. From Penfield/Rasmussen. The Cerebral Cortex of Man. © 1950 Gale, a part of Cengage Learning, Inc. Reproduced by permission. www.cengage.com/permissions
Kellgren differentiated between tenderness within the region to which pain is referred, and “the deep tender spot [that] frequently lies outside the distribution of pain... The patient is unaware of its existence until it is discovered by the physician”, with a “steep rise in pain...which causes the patient to wince and cry out”. (The subjects were volunteer investigators, not “catastrophizing” patients with “fibromyalgia.”)
The value of the “deep tender spots” in diagnosis did not become clear to me until much later, and this did not occur initially in the context of “fibrositis” or “fibromyalgia.” When examining hockey players and dancers, I was often faced with problems of diagnosis for which my medical training had left me unprepared. The bigger problem was not “medically unexplained symptoms,” but firmly held wrong diagnoses and ineffective therapy. If lateral elbow pain subsided with time and an injection, well and good. But multiple recurrences demanded fresh approaches; among other possibilities, perhaps the injection was in the wrong place.
A physiatrist, Max Desmarais, carefully described to me that the tenderness associated with lateral elbow pain was not at the lateral epicondyle, but distally, in the origin of the long extensor to the third finger from the lateral intermuscular septum. It moved with the muscle as the forearm was rolled from pronation to supination. It was not an enthesitis, and was not central to the perceived pain. Injection of anesthetic at this precise site (using small volumes to avoid a field block) relieved the local symptoms and tenderness. It behaved like the “deep tender spot” described by Kellgren as a feature of referred pain. Similarly close examination revealed other sites with similar characteristics. But these alone did not help in “ascertaining the anatomical source of [the] pain.”
MULTIPLE TENDER SITES, ASYMMETRICALLY CLUMPED
Lateral elbow pain was often associated with neck pain. Multiple other sites (mid-trapezius, coracoid tip, second costochondral junction, lateral pectoral site, supraspinatus origin) may also reveal characteristic deep tenderness. Commonly the pain is asymmetrical; and the pattern of referred tenderness is similarly asymmetrical, forming a clumped pattern of “deep tender spots” of which the patient is unaware: strong clues that the pain is cervical in origin.
ORIGIN IN THE LOW CERVICAL SPINE
It took me over 2 decades9,10 to learn how to examine the neck, and many well trained rheumatologists have not (yet) followed. Let me describe the process in loving detail. The relaxed, non-weight-bearing neck has a free range of movement, and in the absence of pathology, allows the examiner to painlessly glide or tilt one vertebral body over another. With the patient supine (not seated — this tightens antigravity muscles), deep structures can be palpated and moved. The long transverse process of C2 is felt behind the angle of the jaw and below the mastoid process. Counting down the transverse processes leads to the transverse process of C4, about halfway between the mastoid process and the clavicle. Rotate the head away from the side being examined to relax the sternomastoid, and gently move the neck to identify the intervals between the separately moving transverse processes. With the head of the examiner’s second metacarpal supporting the fifth transverse process, the tip of the index finger identifies the apophyseal joint for that level posteriorly, testing for any tenderness or pain on movement (an uncommon finding). Anteriorly, the C5–6 disc is identified by the examiner’s thumb, more clearly during passive movement. The 6–7 space may also be identified in turn: lying behind the lower sternomastoid muscle, just above the inner half-inch of the clavicle. The intertransverse ligaments and disc spaces are often tender, but the maximum tenderness is found in the bone and attached structures at the anterolateral corners of the C5 and C6 vertebral bodies: exactly where radiological examination will show osteophytes late in life. The localized tenderness long precedes radiographic change. The patient is never aware of these sites of marked tenderness, and the pain induced by palpation vanishes when the examiner’s thumb is removed, or shifted away. Stand the patient before a mirror to teach the exact location of these key sites, to which treatment must be directed.
For treatment, colleagues had urged the use of neck support during sleep since the 1950s, but it was not until the 1980s that we learned the problem of the high shoulder blocking access to the very lowest part of the anterior cervical spine. During this time I was reviewing patients previously seen with fibromyalgia (FM), in preparation for what became the 1990 American College of Rheumatology study11. Many of these patients, still with neck and upper body symptoms, had lost the tenderness in the upper body sites that became incorporated into the criteria set. They were no longer tender at mid-trapezius, lateral elbow, second costochondral, and supraspinatus sites. They remained very tender in the very lowest part of the cervical spine, and had a new, often asymmetrical pattern of referred tenderness, at origin and insertion of pectoralis minor and inner rather than outer elbow. Once this pattern was recognized, and the treatment strategy revised, a prospective study with new patients was begun, leading to the favorable results published in the C6–7 Syndrome paper12, and a controlled trial in London, Ontario, Canada, using remote patients and independent trialists13.
THE NEUROLOGY OF THE SYMPTOM PATTERN
When pain has its origin in the low neck, the referred symptoms may include headache, pain in the back of the neck spreading towards the shoulder, and pain in the front or back of the chest wall, and down the arms to the hands. Associated symptoms often include blurred vision, or “dizziness,” better described as a momentary sense of imbalance, as there is rarely a spinning sensation.
Equally remarkable is the absence of pain and of tenderness in structures that are highly sensitive, and richly represented in the cerebral cortex. Jaw pain is common, and implicates the mandibular division of the trigeminal nerve, but the pain is confined to the region above the angle of the jaw. The lips and chin have the same nerve supply and are asymptomatic. Recent studies by Starz and his colleagues have confirmed the absence of pain and tenderness in lips, ears, nose, and tongue in most patients with FM14. The pain is widespread, but not diffuse or generalized.
None of this can be explained by the distribution of a single nerve, or even of a single segment. The anatomy of the pattern is determined by the neurology of eye-hand coordination. The nerve cell bodies that receive messages from the region around and above the eyes are located in the spinal cord (and cortex) within an inch of the nerve cell bodies that receive messages from the hands, and from all of the muscles that control the position of the skull, shoulders, and shoulder blades.
EVOLUTIONARY PERSPECTIVES
About 4 million years ago, some small-brained creatures began to walk erect. Why did they do it? They couldn’t run faster or walk further than their predators. But it gave them the use of their hands. Major anatomical changes occurred; a long, strong thumb, a flat, broad ribcage, a reengineered scapula, and a long collar bone. But the broad shoulders made their necks vulnerable when they slept on their sides, and the erect posture led to a hyperextended low back. Great neuromusculature changes evolved.
A few million years later, they could make hammers, or spears, or axes. Soon, they could (and did) chop down trees, and make houses, or boats, or chop down more trees, and make war, or places of worship. Jared Diamond in Collapse16 has documented all this.
Writing followed, so knowledge could be passed through generations — unless books went out of print, or were unread. The relationship between tender points and referred pain was described, but then lost. Rheumatologists wouldn’t or couldn’t do point counts, so tender points were declared obsolete16. Now primary care physicians can label “fibromyalgia” as well as rheumatologists, and can dismiss the patients to clinics for “multidisciplinary care.” And the last tree was cut down on Easter Island.
MULTIDISCIPLINARY CARE
With training, physiotherapists can be as skilled as any physician. Unfortunately, they work in clinics under the same time pressures as their MD colleagues. The Institute for Work and Health in Ontario, Canada, performed a prospective study of 1600 injured workers off work because of “soft-tissue” musculoskeletal problems, followed for one year. About half were treated at 100 community-based Compensation Board-sponsored multidisciplinary clinics, stressing early active exercise and education programs; the remainder received usual care. Some clinics were based in teaching hospitals; others offered accessible physiotherapy, chiropractic, or multiple services. Functional status, health-related quality of life, and pain measures all improved significantly throughout time, but there were no statistically significant differences in rate of improvement between the 2 groups. Healthcare costs for clinic attenders were much higher17. The assignments were not random, but no study with comparable power has substantiated superior results of “multidisciplinary” care for “fibromyalgia,” or any other “soft tissue pain syndrome.” Improvement is strongly related to time, a factor not routinely factored into metaanalyses. Elimination of these ineffective and very costly programs has proved politically impossible.
PHARMACOTHERAPY
We are trying very hard. There are many agents; patients receive some benefit, but when side effects make the patient tired, dull, lethargic, and fat, neither their goals nor those of society are satisfactorily met. But the astonishing results of treatment of rheumatoid arthritis with tumor necrosis factor (TNF) blockers, plus the systemic difficulties in achieving recognition and treatment of referred pain syndromes, means that the search must continue. Scholars of despair may review the New England Journal of Medicine, issue of 18 December 2008, with articles on noninfectious chronic pelvic pain in men, and temporomandibular dysfunction. Both concede that etiology is unknown, but the authors of neither article conceive of the possibility of referred pain mechanisms.
IS FM PAIN “LEGITIMATE” OR JUST A LABEL?
Dr. Wolfe suggests that the legitimacy of “fibromyalgia” rests on “a single partially objective sign — tenderness on palpation.” A (too?) strict definition of the syndrome has been essential for any of the landmark studies. Apart from the sleep EEG abnormalities18–21 there is now a wealth of laboratory evidence of activation of pain pathways. Strangely, his extensive bibliography omits Vaeroy’s description of elevated levels of substance P in the cerebrospinal fluid22, confirmed and extended to other neurotransmitters in the pain pathway by Russell and others23. Further, the literature has exploded since the description of complex changes in patterns of cerebral blood flow revealed by functional magnetic resonance imaging24, as applied to FM and other acute and chronic pain syndromes.
There is also a rich neurosurgical literature derived from the use of microelectrode recording and microstimulation during functional stereotactic mapping, primarily for the study and treatment of movement disorders and pain syndromes, but also used for the anatomical mapping of pain pathways25–27. Early work had suggested that pain and temperature inputs were processed in the thalamus, and detailed studies mapped out a rough equivalent of the Penfield homunculus. Peripheral stimulation activated thalamic cells, and thalamic stimulation caused peripheral sensations.
In 2001, Wallace hypothesized that cytokines may play a role in the pathogenesis of FM, but was not able to support this in a small pilot study28. In rats, intrathecal TNF blockade had been shown to be effective in blocking neuropathic pain29. In humans, Wallace’s suggestion was supported in a larger, controlled study of cytokines including TNF in FM30. In a smaller study, circulating cytokine levels were followed over a 6-month period31. With time and “multidisciplinary” therapy (not including TNF blockers), levels of TNF-α fell. In the past decade, scores of thousands of patients with rheumatoid arthritis have been treated with TNF-blocking agents, with striking relief of pain and other “fibromyalgia-like” symptoms. Given selection pressures, many of these would have had FM or related symptoms, but fewer tender points. That the research protocols did not include point counts is, to me, reprehensible.
The label “fibromyalgia,” strictly defined, accommodates and gives meaning to all of the related symptom complexes, which may be present in patients who do not quite meet the 1990 criteria. These identify a mountain, surrounded by some very large molehills. But if the entire mountain is dismissed in terms such as Somatoform Disorder, Hysteria, Psychological Distress, Mental Distress, Psychiatric Disorder, and Health-Care Seeking Behavior, the interactions among physicians, students, patients, researchers, and insurers become dysfunctional.
But Dr. Wolfe knows all this. He has been partnered with “fibromyalgia” for about 30 years. The community rheumatologists on whom he depends won’t or can’t do point counts.
Let us assume the best of motives and of competence, on the part of the patients and their medical advisors. It takes only about 20 minutes with a mentor to learn how to do a count of tender sites, and appropriate control sites. It takes about the same length of time with a patient to ask the questions, listen carefully to the answers, and perform the examination. At the end of this time, the advisor can know the interactions between mechanical problems, amplifying factors, and concomitant medical conditions.
But the gain at this point is zero. It does not help that the advisor knows what is to be done; the patient must know, must have it explained and demonstrated in full detail, supported by handouts and a careful letter to the referring physician (another hour). Because referred pain by its nature is nonintuitive, and treatment response is relatively slow, reinforcement is essential, by the original advisor in followup or by an appropriately trained surrogate. The economics of all this are rarely feasible. Easier to give “reassurance,” a label, and a pill.
Could it be better? The answer is yes.
Footnotes
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.