

A 28-year-old woman with 10-year history of poorly controlled “schizophrenia” was admitted because of intermittent fever and diarrhea. Limb weakness developed shortly after admission, but initial magnetic resonance imaging (MRI) showed no central nervous system abnormality. Acute renal failure with nephritis and symptomatic pulmonary embolism developed within 5 days. Laboratory studies revealed high-titer lupus anticoagulant, anti-ß2-glycoprotein I, and multiple autoantibodies, including anti-double- stranded DNA. In addition to systemic lupus erythematosus (SLE), probable catastrophic antiphospholipid syndrome (APS) was diagnosed for the typical clinical features, but with no histological confirmation of microthrombosis1. Pulsed cyclophosphamide with enoxaparin was given, but the patient’s consciousness dramatically deteriorated from clear to comatose within 1 day. Repeated head MRI (Figure 1) showed diffuse and marked cortical edema, with herniation compressing the brain stem (arrow, Figure 1A). The acute cortical edema was attributed to ischemic change because of the characteristic distribution in parallel with vascular territories in bilateral fronto-parietal areas complicated with mild hypothalamic hemorrhage (arrow, Figure 1B). The patient succumbed to the refractory disease shortly afterward.
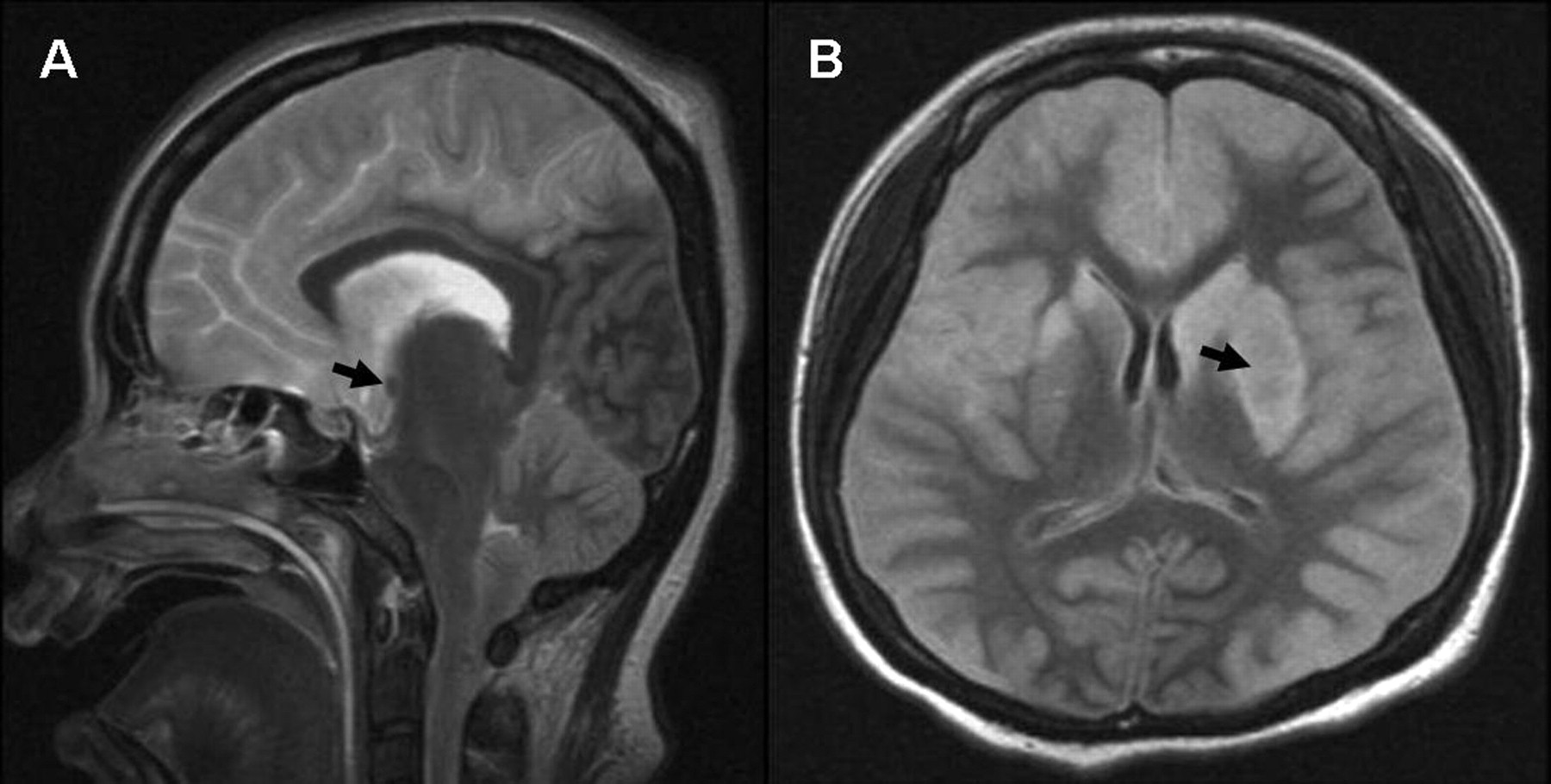
A. T2-weighted MRI shows diffuse and marked cortical edema, with herniation compressing the brain stem (arrow). B. FLAIR image shows mild hypothalamic hemorrhage (arrow).
Catastrophic APS features diffuse microvascular thrombosis affecting multiple organs over days or weeks, which can be triggered by infection and lupus flares, as probably occurred in this case1–4. Although cerebrovascular involvement is common in catastrophic APS2,4, diffuse bilateral cortical ischemia, which may be a manifestation of multiple cerebral microvascular thrombosis, has never been reported. The longterm psychosis in this patient could have been a neuropsychiatric manifestation of previously unrecognized SLE, which is also associated with antiphospholipid antibodies5.








{kind=link}