
Abstract
Objective. To evaluate if serum concentrations of osteopontin (OPN) at baseline in patients with juvenile idiopathic arthritis (JIA) represent a potential predictor of responsiveness to methotrexate (MTX).
Methods. At diagnosis, 60 children with active JIA received MTX in addition to nonsteroidal antiinflammatory drugs. After 12 months of MTX treatment, 30 patients were defined as responders; the 30 nonresponders received anti-tumor necrosis factor-α therapy (etanercept) in addition to MTX; this group was then enrolled for an additional 12-month study period. No patient had received steroids within 6 weeks before entering the study. Fifty healthy children matched for sex and age acted as controls. OPN serum levels were measured at baseline, before MTX, and then at 6 and 12 months. In the nonresponder patients, OPN was evaluated again after 6 and 12 months of etanercept treatment.
Results. At baseline, OPN values were significantly higher (p = 0.0003) in JIA patients than in controls, with no significant differences among the different JIA subtypes. At baseline, OPN levels were lower in responders than in nonresponder patients (14.16 ± 10.1 μg/ml vs 33.2 ± 18.1 μg/ml, respectively). After 12 months of MTX treatment, OPN levels were significantly reduced in comparison to baseline in both responder and nonresponder groups (p = 0.0017, p = 0.0048, respectively). In nonresponders, etanercept significantly reduced OPN levels at 6 and 12-month followup in comparison to baseline (p = 0.002, p = 0.008, respectively). No significant differences were found among OPN levels and disease activity.
Conclusion. Serum levels of OPN at baseline represent a possible marker to predict the responsiveness to MTX in patients with JIA.
- OSTEOPONTIN
- MARKER
- METHOTREXATE
- JUVENILE IDIOPATHIC ARTHRITIS
Juvenile idiopathic arthritis (JIA) includes a heterogeneous group of chronic arthritides of unknown origin occurring before 16 years of age. Although the etiology and pathogenesis of JIA are unknown, there is evidence that T cell-mediated inflammation plays an important role in enabling chronic synovitis1.
Osteopontin (OPN), a secreted phosphoglycoprotein of approximately 300 amino acid residues, is highly expressed in bone, where it promotes adhesion of osteoclasts to the mineralized matrix regulating bone resorption and formation2. OPN expressed in T cells early in the course of bacterial infections3 is a proinflammatory molecule promoting cellular homing and releasing proteinolytic enzymes4–6. OPN is physiologically secreted by a variety of cells including macrophages, activated T cells, smooth muscle cells, and epithelial cells7. In the inflammatory context, it is mainly expressed by natural killer and activated T cells, playing a critical role in the production of many inflammatory factors like cytokines and chemokines in Th1-mediated cellular immunity8,9. Recent studies support an important role of OPN in inflammatory arthritis10, being significantly overexpressed in synovial T cells derived from patients with rheumatoid arthritis (RA), at the level of both mRNA and protein3,11–13. Among patients with RA there is a large degree of interindividual variability of response to treatment with methotrexate (MTX), although the factors responsible for the efficacy of the drug are unknown. Studies have shown that gene polymorphisms can influence the response to MTX or to etanercept, providing a potential mechanism for identifying patients who are more likely to benefit from these therapies14–16.
Given the key role of OPN in inflammatory arthritis, our aim was to assess the possible role of the serum OPN profile as a predictive marker of responsiveness to MTX in a cohort of patients with JIA at disease onset, before they started therapy with any disease modifying antirheumatic drug.
MATERIALS AND METHODS
A cohort of 60 consecutive children (41 girls, 19 boys, median age 9.7 ± 2.6 yrs) attending the outpatient clinic of the rheumatology units at the departments of pediatrics of the universities of Florence and Padua, and fulfilling the International League of Associations of Rheumatology criteria for the diagnosis of JIA17, were prospectively enrolled (15 with extended oligoarticular disease, 8 persistent oligoarticular, 2 psoriatic, 30 polyarticular rheumatoid factor (RF)-negative, and 5 systemic with polyarticular course). Patients’ demographic data and measures of disease activity are summarized in Table 1.
Demographic characteristics and measures of disease activity and improvement from baseline to 1-year followup in 41 girls and 19 boys.
At diagnosis of JIA, all patients received nonsteroidal antiinflammatory drugs, and then 3–6 months later, MTX (10 to 12.5 mg/m2 of body surface area per week) was introduced18. No patient was receiving or had received either oral or intravenous steroids at least 6 weeks before entering the study.
Enrollment criteria included active disease defined as the presence of at least 2 active joints (joints with swelling or, in the absence of swelling, with limited motion and pain or tenderness or both) in the case of persistent oligoarticular JIA, and 5 active joints in the other types of JIA onset19.
Patients were defined as responders or nonresponders if they satisfied the American College of Rheumatology Pediatric 50 (p-ACR 50) definition of improvement (at least 50% of improvement response from baseline in at least 3 of any 6 core set variables with no more than one indicator worsening by more than 30%)19.
Fifty healthy children matched for sex and age living in the same geographic area (32 girls, 18 boys, median age 8.9 ± 2.1 yrs) served as controls after the exclusion of rheumatic, metabolic, and endocrine diseases. All patients and controls were prepubertal.
Blood samples were collected sequentially during routine laboratory tests by antecubital venepuncture. Sera obtained by centrifugation were stored at −70°C until measurement. OPN was measured at baseline before patients started MTX, then at 6 and 12 months. In nonresponder patients serum levels of OPN were measured consecutively after 6 and 12 months of etanercept therapy. The core set criteria for disease activity were evaluated at the same time.
Approval for the study was obtained by the ethics committees of A. Meyer Hospital, Firenze, and Padua Pediatrics Department, Padova; parents gave their informed consent.
Measurement of serum OPN
Serum concentrations of OPN proteins were measured quantitatively by ELISA (Immunodiagnostik, Benshein, Germany) according to the manufacturer’s procedure. The OPN ELISA kit was purchased from Assay Designs and was designed by the manufacturer to specifically detect the noncleaved form of OPN. The kit was also evaluated for serum assay. Microtiter plates precoated with purified mouse antibodies against the OPN were washed and nonspecific binding sites were saturated with 10% (wt/vol) fetal bovine serum for 1 h and subsequently washed. Serum was diluted with phosphate buffered saline and added into duplicate wells and plates were incubated 2 h. Then color development was stopped and the color intensity was measured. OPN serum values were expressed in g/ml as mean ± SD of the plasma values. Investigators responsible for the OPN analysis were blinded to the responder/nonresponder status of the patients.
Statistical analysis
Mann-Whitney U test and analysis of covariance (ANCOVA) with least significant difference correction were used to evaluate the OPN differences between responders and nonresponders. Spearman rank correlation test was used to determine correlation coefficients among OPN and core set activity indexes. During ANCOVA analysis we considered several covariates: sex, age, pubertal stage, body mass index (BMI), and disease duration. This selection was made because several factors could potentially modify plasma and/or serum levels of OPN. In particular, factors related to growth–plate ossification such as OPN are upregulated during the “catch-up” process. For these reasons we considered age, pubertal status, and sex as important covariates able to influence the results. In addition, several studies have demonstrated a correlation between plasma OPN and body weight and BMI in both animal and human models19. Nonparametric tests were used, where necessary, due to the small size of our groups and the skewed characteristic of our data. A forward stepwise multiple logistic regression analysis was used to elucidate any association between serum OPN, erythrocyte sedimentation rate, hemoglobin, or C-reactive protein and the response to therapy. Levels of p < 0.05 were considered statistically significant. The StatSoft 5.1 statistical package (StatSoft Inc., Tulsa, OK, USA) was used.
RESULTS
At baseline, OPN values were significantly higher in JIA patients than in controls: 22.3 ± 17.8 μg/ml versus 4.18 ± 1.2 μg/ml, respectively (p = 0.000013; Figure 1A). No significant differences were observed in the levels of serum OPN among the different JIA subtypes.
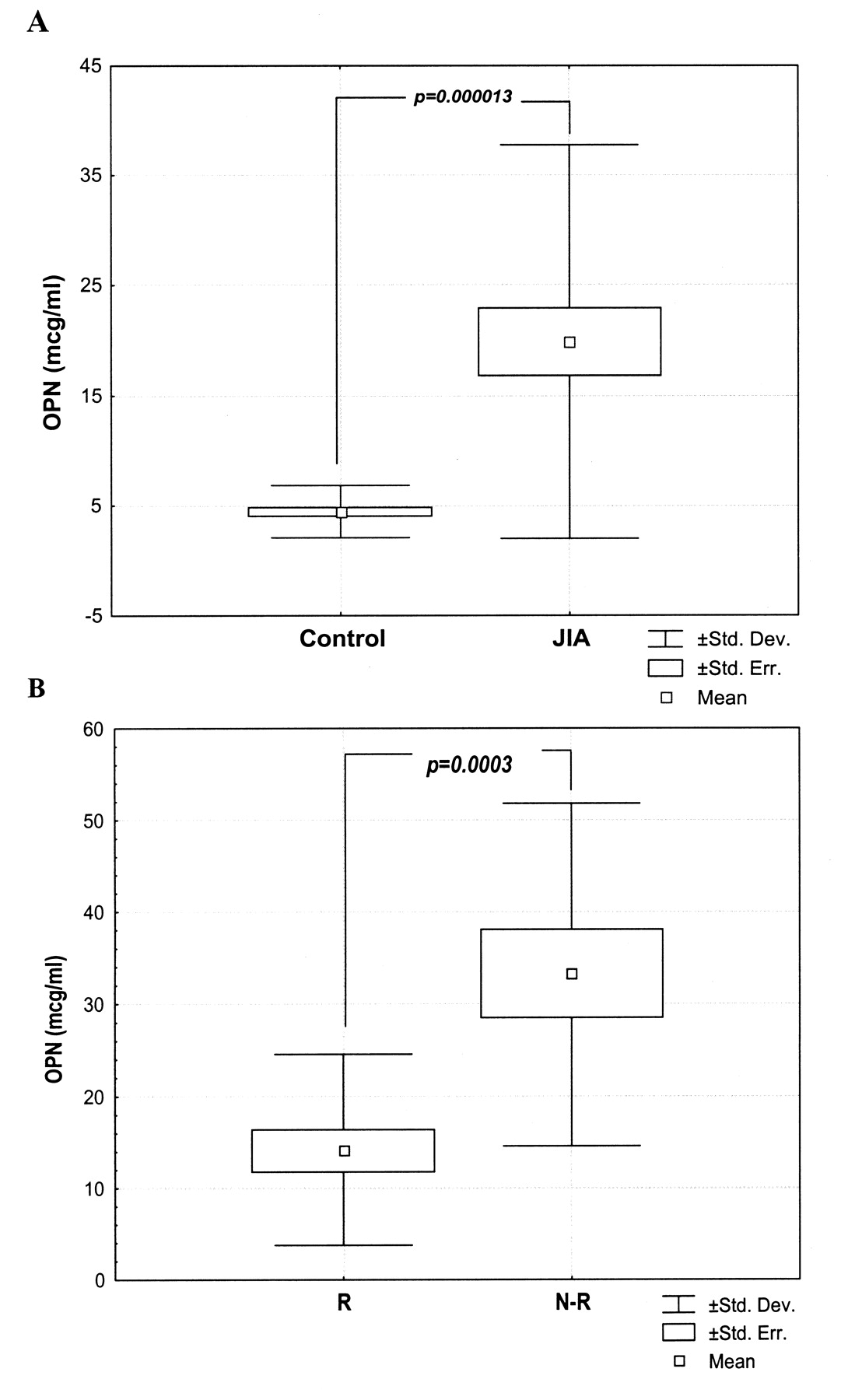
Serum OPN values at baseline. A. Values were significantly higher in JIA patients than in controls. B. Levels were significantly lower in the responder (R) patients compared to the nonresponders (N-R).
After 12 months of MTX therapy, according to the definition of improvement19, patients were divided into 2 groups: Group 1, the responders (18 girls, 12 boys, mean age 8.6 ± 1.9 yrs), included 12 polyarticular RF-negative, 10 extended oligoarticular, and 8 persistent oligoarticular JIA patients; and Group 2, the nonresponders (23 girls, 7 boys, mean age 10.1 2.3 yrs), included 18 polyarticular RF-negative, 5 systemic and polyarticular course, 2 psoriatic, and 5 extended oligoarticular JIA patients. Twenty-five (42%) of the 60 patients met the definition of 30% improvement, 22 (36%) achieved 50% improvement, and 8 (13%) achieved 70% improvement at the end of the study, while 5 (8%) were nonresponders. All 30 nonresponder patients received anti-tumor necrosis factor-α (anti-TNF-α) therapy (etanercept, 0.4–0.6 mg/kg body weight, subcutaneously twice weekly) in addition to MTX; this group was then enrolled for an additional 12-month study period.
At baseline, we observed statistically significant lower levels of serum OPN in the responder compared to the non-responder patients, 14.16 ± 10.1 μg/ml versus 33.2 ± 18.1 μg/ml, respectively (p = 0.0003; Figure 1B).
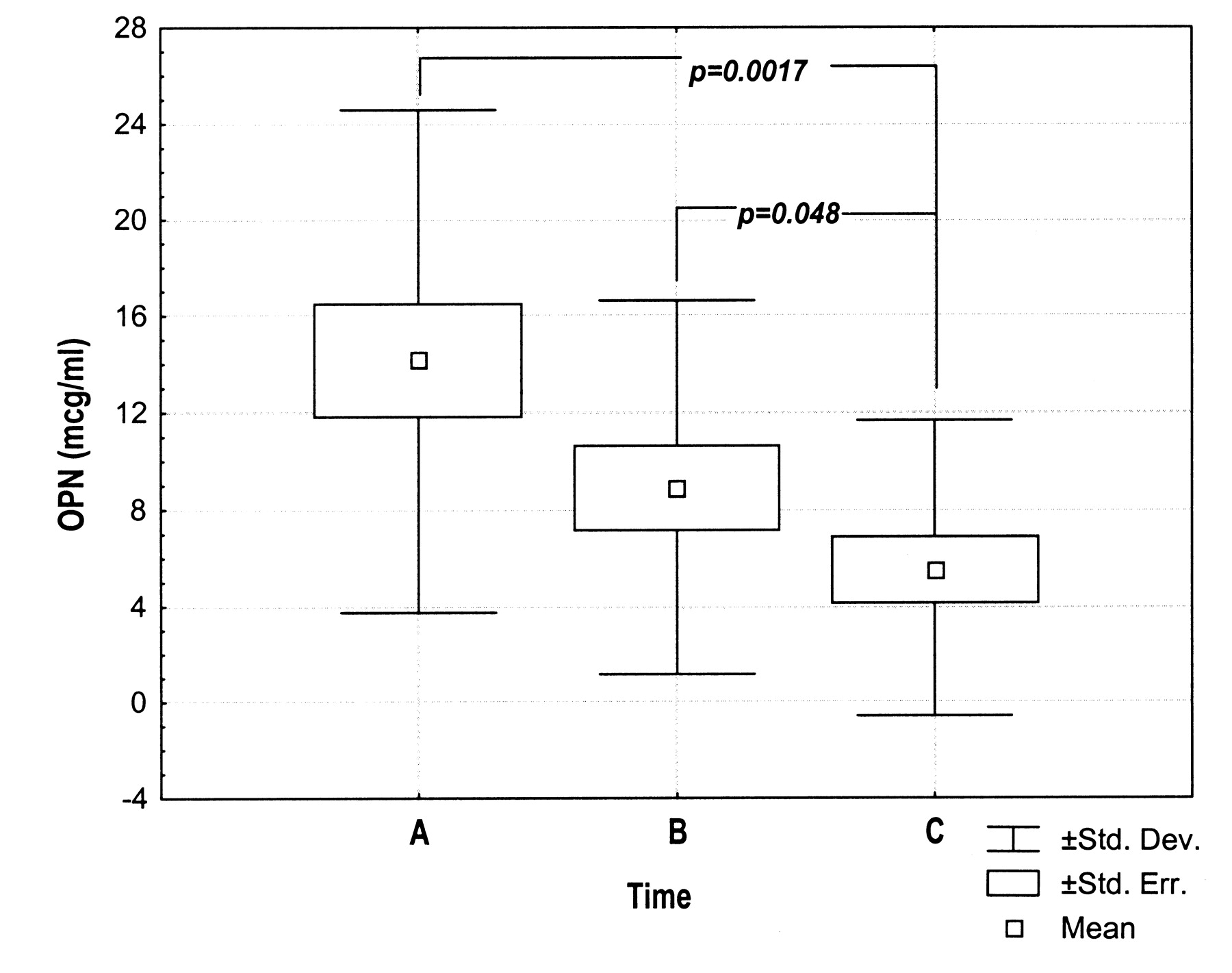
Over 12 months of MTX therapy, OPN serum levels showed no significant differences in the whole group of JIA children or in nonresponders. A significant trend was observed among the responder patients (p = 0.006, ANCOVA). Indeed, the least significant difference test showed a significant reduction of serum OPN in the responder group after 12 months of MTX therapy. In particular, serum OPN levels were significantly lower after 12 months of MTX therapy in comparison with 6 months of MTX therapy, 5.5 ± SD 6.5 μg/ml after 12 months compared to 8.89 ± SD 7.7 μg/ml after 6 months (p = 0.048), and compared with 14.16 ± SD 10.1 μg/ml at baseline (p = 0.0017; Figure 2).

In the responder group, serum OPN levels were significantly lower after 12 months of MTX therapy (“C”) in comparison with baseline values (“A”) and 6 months of MTX therapy (“B”).
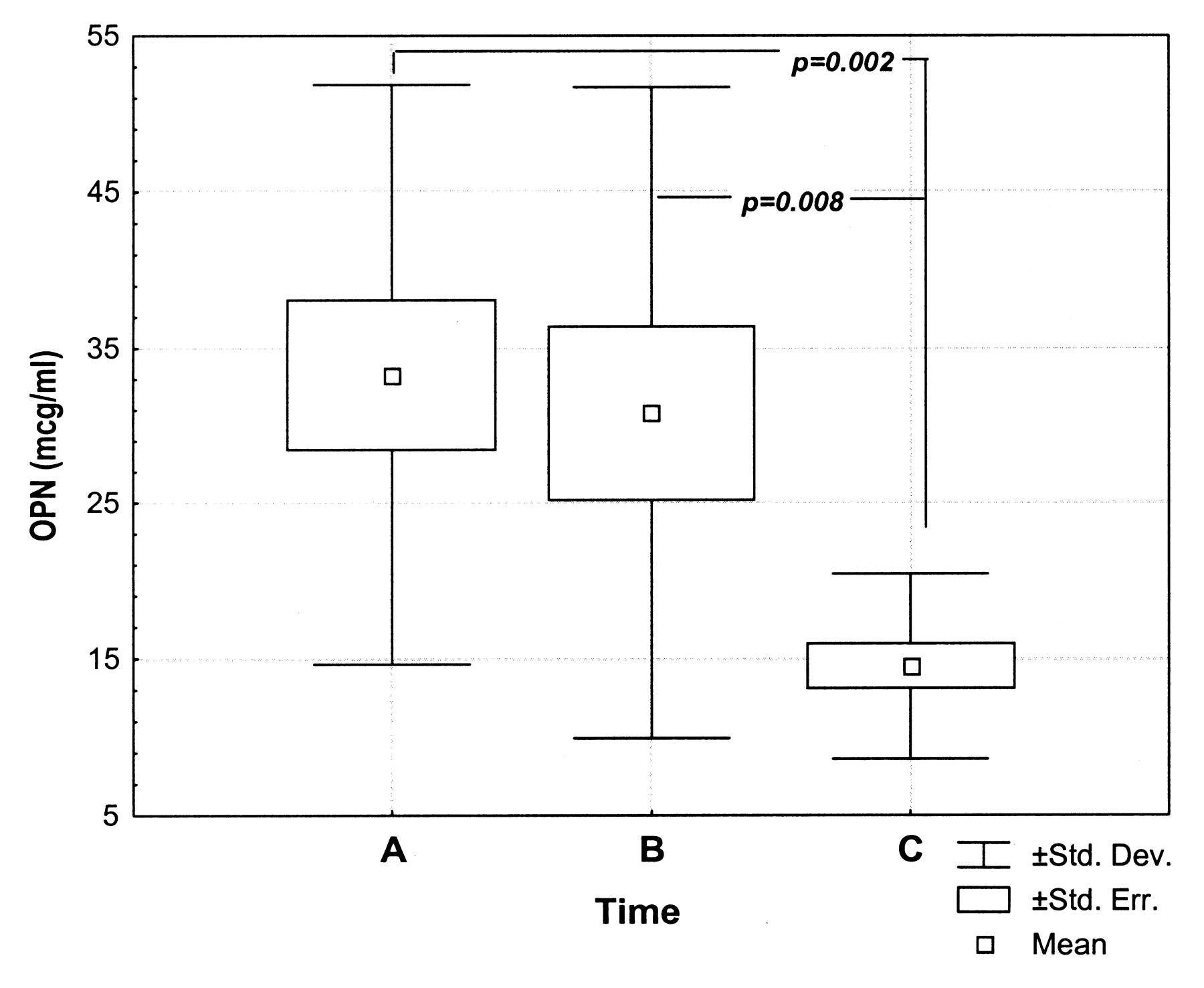
The MTX nonresponders showed decreased OPN levels after 6 and 12 months of etanercept therapy. This decrease was not significant at 6 months (33.2 ± 18.1 μg/ml baseline vs 30.8 ± 20 μg/ml at 6 mo); however, at 12 months OPN values were significantly reduced in comparison to baseline and 6 months (14.5 ± 5.9 μg/ml at 12 mo, compared to 33.2 ± 18.1 μg/ml at baseline and 30.8 ± 20 μg/ml at 6 mo; p = 0.002, p = 0.008, respectively; Figure 3).

{kind=link}
{kind=link}
{kind=link}
In the nonresponder group, OPN values were significantly lower after 12 months of MTX + etanercept therapy (“C”) in comparison with baseline values (“A”) and 6 months of MTX + etanercept therapy (“B”).
No significant differences were found among OPN levels and the index activity core set criteria. In multiple logistic regression analysis we observed that OPN and hemoglobin levels were the 2 relevant predictors for response to therapy (p = 0.001 for OPN; p = 0.021 for hemoglobin). Table 2 gives the beta-coefficients and p values of the factors we analyzed.
Factors associated with response to the therapy: multiple logistic regression analysis.
DISCUSSION
We observed that serum concentrations of OPN were significantly higher in children with JIA than in controls. As reported6, these data seem to provide additional evidence of a potential role of OPN in the inflammatory process. It has been observed that OPN mRNA and protein are overexpressed in synovial tissue from patients with RA and trigger the production of various proinflammatory chemokines5. The higher amounts of serum OPN in patients with JIA may be an index of high cartilage and bone turnover and joint destruction. In contrast to our results, Ohshima, et al found no significant differences in serum OPN levels among RA patients and healthy controls4. We may speculate that age could influence the rate of cartilage and bone destruction. OPN is an important factor regulating both physiological and pathological mineralization and bone remodeling7. It is involved in the regulation of bone resorption: OPN-knockout mice are markedly protected from bone loss following ovariectomy20. The higher serum levels of OPN in children with JIA could reflect a higher rate of bone resorption and a reduction of bone mass. In addition, OPN inhibits the formation of hydroxyapatite, and higher levels in patients with JIA may significantly affect bone mineralization21.
Our study population included patients with different JIA subtypes. Oligoarticular JIA can follow a persistent or an extended course. Patients with systemic-onset disease usually have a polyarticular course when systemic features (fever and rash) disappear; patients with psoriatic arthritis usually experience a polyarticular involvement. Contrary to our expectation, no significant differences of serum levels of OPN were found in the different subtypes.
Considering the response to MTX, we found significantly higher OPN levels in nonresponders than in responder patients at baseline. These results suggest OPN as a potential tool to discriminate responders from nonresponders in patients receiving MTX. After 12 months of MTX treatment, responders showed a significant decrease of serum OPN compared to baseline. This OPN serum profile might help in differentiating patients who will respond to MTX from those who will not respond and who thus could require treatment with biological agents. It is known that other factors including subtype of JIA and number of active joints may interfere with responsiveness to MTX. However, at onset we were unable to predict those who would or would not respond to MTX. We observed that patients with responsiveness to MTX had lower levels of OPN at baseline compared to nonresponders. Hence, the persistence of high levels of OPN in JIA patients could represent a potential predictor of disease severity.
All nonresponder patients underwent etanercept treatment in addition to MTX; at the one-year followup a significant reduction of OPN levels was observed, again emphasizing the role of the serum profile of OPN as a potential predictor of responsiveness to therapy. Further, these results seem to highlight the role of OPN as an independent index, apparently unrelated to disease activity scores. Alternatively, the higher OPN levels in MTX nonresponders may point toward persistent active disease. It is well known that OPN is able to induce the expression of proinflammatory chemokines, enhances the expression of receptor activator of nuclear factor-κB ligand (RANKL), and decreases the expression of osteoprotegerin11. Patients with persistent high levels of OPN after one year of MTX therapy could probably produce larger amounts of RANKL, and treatment with anti-TNF-α could inhibit osteoclast activity, thus reducing OPN levels.
Together, these data point to OPN as a potential index of inflammatory processes in JIA. OPN reduction during therapy with either MTX or etanercept in children with JIA might be a potential indicator to evaluate the responsiveness to treatment. Notably, OPN concentrations at disease onset might be a key predictor of JIA severity, suggesting a more aggressive therapy independent from the number of joints involved. Indeed, no differences were found among the different subtypes of JIA and the number of active joints. OPN seemed to correlate predominantly with inflammation, as proven by its reduction after initiation of therapy.
Footnotes
- Accepted for publication May 1, 2009.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.