
Abstract
Objective. Aortic pulse wave velocity (PWV) is an independent predictor of risk for atherosclerotic cardiovascular disease. Metabolic syndrome (MetS) is more prevalent in patients with systemic lupus erythematosus (SLE) compared with matched healthy subjects. Aortic PWV is increased in MetS. The purpose of this cross-sectional study was to determine the association between MetS and aortic PWV and other surrogate biomarkers of subclinical atherosclerosis in SLE.
Methods. One hundred twenty-eight patients with SLE were studied. We established the presence of MetS according to the National Cholesterol Education Program Adult Treatment Panel III definition and we measured PWV, glucose, insulin, glycosylated hemoglobin (HbA1c), insulin sensitivity (HOMA index), lipid levels, uric acid, homocysteine, fibrinogen, D-dimer, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), interleukin 6 (IL-6), IL-8, IL-10, C3, C4, autoantibodies, SLE Disease Activity Index (SLEDAI), and Systemic Lupus International Collaborating Clinics/ACR Damage Index. Duration of SLE and treatment was also recorded. Multivariate logistic regression analysis was used to identify independent determinants of increased PWV.
Results. SLE patients with MetS had higher aortic PWV (9.8 ± 2.4 vs 8.5 ± 1.7 m/s; p = 0.002) and increased biomarkers of subclinical atherosclerosis such as CRP, IL-6, C3, uric acid, homocysteine, fibrinogen and D-dimer, compared to those without MetS. HOMA index and insulin and HbA1c levels were also higher in this group. No differences were found in variables related to lupus activity (ESR, C4, SLEDAI, IL-8, IL-10, and treatment for SLE). In the multivariate model, increased PWV was associated with age, male sex, MetS, duration of SLE, and CRP.
Conclusion. MetS may contribute to the development of accelerated atherosclerosis in SLE.
- SYSTEMIC LUPUS ERYTHEMATOSUS
- METABOLIC SYNDROME
- INSULIN RESISTANCE
- ATHEROSCLEROSIS
- PULSE WAVE VELOCITY
Although the exact mechanisms that lead to the development of atherosclerotic cardiovascular disease (ASCVD) in patients with systemic lupus erythematosus (SLE) are not fully established, traditional and nontraditional cardiovascular risk factors appear to be implicated1. Metabolic syndrome (MetS) is defined as a clustering of CVD risk factors, characterized by central obesity, glucose intolerance, hypertension (HTN), dyslipidemia, insulin resistance (IR), and a systemic proinflammatory and procoagulating state2. It is increasingly recognized as an independent predictor of cardiovascular morbidity and mortality3, particularly in women4. A relatively high prevalence of MetS has been observed in patients with SLE5–7. We found a prevalence 3.8 times higher in SLE patients aged ≤ 40 years in comparison with a control group matched for age, sex, and education level7. Moreover, the frequency of ASCVD in the SLE group with MetS was 2.2 times higher than that in the SLE group without MetS, suggesting that MetS by itself may contribute significantly to the development of ASCVD in these patients7.
Recently, several longitudinal studies directly demonstrated that aortic stiffness, measured using carotid-femoral pulse wave velocity (PWV), is an independent predictor of all-cause and cardiovascular mortality, coronary events, and stroke8. Increased vascular stiffness has been found in middle-aged women9,10, adolescents, and young adults with SLE11, and it has been suggested that this condition may be a factor contributing to the increased cardiovascular risk observed in these patients.
Although MetS has been associated with increased arterial stiffness among the general population12,13 and in several patient groups14,15, the influence of MetS on arterial stiffness in SLE has not been well defined. We conducted a cross-sectional study involving a cohort of SLE patients to explore the link between MetS and PWV and other surrogate biomarkers of subclinical atherosclerosis.
MATERIALS AND METHODS
Participants
One hundred twenty-eight patients with SLE that fulfilled ≥ 4 of the American College of Rheumatology 1997 revised criteria16 were recruited from the Autoimmune Diseases Unit of our hospital. All participants were White. We excluded SLE patients who had not been monitored for at least 1 year in our unit and patients with a suspected active infection or other disease involving systemic inflammation, except SLE, at the time of inclusion. Patients with ASCVD were also excluded. All participants gave informed consent to participate in this study, which was approved by the local ethics committee.
Protocol and clinical assessment
This was a cross-sectional study conducted over a 4 month period. Patients attending a scheduled visit over the period of the study were assessed for traditional CV risk factors, demographic and education data, comorbidities, and current medications. Other demographic and clinical data were obtained from the medical records in a computer database. Clinical definitions are summarized in the Appendix. Patients were defined as having MetS according to the National Cholesterol Education Program Adult Treatment Panel III (ATP III) definition19 (Appendix). Disease activity and accumulated organ damage were measured with the SLE Disease Activity Index (SLEDAI)20 and the Systemic Lupus International Collaborating Clinics/ACR Damage Index (SDI)21, respectively.
Laboratory assessment and assessment of IR
Fasting blood samples for biochemical and immunological tests were collected the day after the scheduled visit and processed routinely the same day, using techniques as described7. Other measures studied were glycosylated hemoglobin (HbA1c; by high performance liquid chromatography, HA-8160, Menarini Diagnostics, Florence, Italy); fibrinogen (von Clauss assay); D-dimer (ELISA, Dimertest, Agen Biomedical, Brisbane, Australia); homocysteine (AxSYM Homocysteine; Abbott Laboratories, Abbott Park, IL, USA), and plasma insulin (BioRad, Marne-la-Coquette, France).
HOMA index for IR was calculated according to the formula in the HOMA model22. Arbitrarily, SLE patients with a HOMA index value that exceeded the 75th percentile of patients included in the study (≥ 2.51) were classified as having increased IR.
Cytokine measurements
Plasma and serum were separated by centrifugation and stored at −70°C. IL-6 serum concentration was measured by immunoradiometric assay using commercial kits (BioSource Europe, Nivelles, Belgium). Similarly, plasma IL-8 and IL-10 levels were estimated using commercial ELISA kits (R&D Systems, Minneapolis, MN, USA) following the manufacturer’s instructions. The intra- and interassay coefficients of variation for biomarkers were IL-6, 4.3% and 2.3%; IL-8, 6.3% and 8%; IL-10, 3.2% and 4.3%, respectively.
Pulse wave velocity measurement
Arterial stiffness was evaluated by measuring carotid-femoral (aortic) PWV using an automatic device (Complior; Colson, Createch Industrie, France) by a single blinded researcher (JAVH) unaware of patients’ MetS status. Two pressure waves were recorded tran-scutaneously at the right common carotid artery and over the right femoral artery. PWV was established as the foot-to-foot velocity. Pulse transit time was established as the average of 10 consecutive beats. The distance travelled by the pulse wave was measured over the body surface as the distance between the 2 recording sites. Aortic PWV was automatically calculated as the ratio of distance to transit time [PWV = D/t(m/s)]. The validation of this automatic method and its reproducibility has been well established23. We arbitrarily defined an abnormally increased PWV as the value exceeding the 75th percentile of SLE patients included in the study (≥ 9.67 m/s).
Statistical analysis
The data are presented as the median (range) for continuous variables and percentage for categorical variables. Differences between continuous variables were tested for significance using the Mann-Whitney test. Categorical data was analyzed using Pearson’s chi-square test. Categories of HOMA index were defined as presence of IR (HOMA index ≥ 2.51) or absence of IR (HOMA index < 2.51). PWV was categorized as increased arterial stiffness (PWV ≥ 9.67 m/s) or normal arterial stiffness (PWV < 9.67 m/s). A multivariate logistic regression analysis was used to identify independent determinants of increased PWV (dependent variable) in SLE patients. The independent determinants tested were age, sex, HTN, MetS, C-reactive protein (CRP) level, uric acid level, hydroxychloroquine (HCQ) use, HOMA index, and SDI. All analyses used a 5% two-sided significant level. Statistical analyses were carried out using SPSS software for Windows (version 14.0; SPSS Inc., Chicago, IL, USA).
RESULTS
One hundred twenty eight patients with SLE (88% women; median age 40 yrs, range 16–78 yrs) were studied. Twenty-six (20%) were diagnosed as having MetS, a frequency similar to that previously found in our SLE cohort7. The median disease duration in this SLE cohort was 11 years (range 1–50), median age at disease onset was 28 years (range 11–76), and the median education level was 8.5 years (range 0–17). Forty-six patients (36%) had renal involvement and 19 (15%) experienced neurological manifestations. The median SLEDAI value for all patients was 4 (range 0–18), indicating that most patients had inactive or moderately active disease status. The median SDI was 1 (range 0–8). At the time of recruitment 88 (69%) patients took prednisone, 95 (74%) received hydroxychloroquine (HCQ), and 43 (33%) were receiving immunosuppressive therapy (1, periodic treatment with intravenous cyclophosphamide because of active lupus nephritis; 7, mycophenolate mofetil, median 750 mg/day; 10, methotrexate therapy, median 10 mg/wk; and 25, azathioprine, median 100 mg/day). In order to establish the presence of MetS in this series, we established 2 categories — i.e., with or without immunosuppressive therapy.
Demographic and metabolic differences between SLE patients with and without MetS
The main differences between SLE patients with and those without MetS are shown in Table 1. To summarize, SLE patients with MetS were older, they had a lower level of education, and the age at onset of SLE was higher. As expected, they had higher blood pressure and body mass index, as well as higher levels of fasting glucose, HbA1c, insulin, HOMA index, and triglycerides, and decreased levels of high-density lipoprotein. Low-density lipoprotein levels were also found to be higher in these patients. Consequently, SLE patients with MetS were more likely to suffer from obesity (OR 32, 95% CI 10–99, p < 0.001), HTN (OR 5.3, 95% CI 1.7–16.4, p = 0.002), dyslipidemia (OR 11.4, 95% CI 1.5–88, p = 0.009), diabetes mellitus (OR 24, 95% CI 2.7–99, p = 0.001), and increased IR (OR 4.1, 95% CI 1.6–10.3, p = 0.002).
Demographic, clinical, and metabolic characteristics of SLE patients with and without metabolic syndrome. Values are median (range) unless stated otherwise.
PWV, SLE-related factors, and biomarkers
SLE patients with and without MetS differed significantly with regard to arterial stiffness, given that average aortic PWV was significantly higher in the MetS group compared to the non-MetS group (p = 0.002). Interestingly, inflammatory biomarkers such as CRP and IL-6 and other markers associated with ASCVD including C3 complement, uric acid, homocysteine levels, fibrinogen, and D-dimer concentrations were also significantly higher among SLE patients with MetS (Table 2). In contrast, no differences in ESR, IL-8, and IL-10 were found (Table 2). Hemoglobin levels and white blood cell counts were also similar in both groups, as well as the autoantibody pattern (anti-nDNA, Ro, La, RNP, and antiphospholipid antibodies; data not shown).
Pulse wave velocity, inflammatory, prothrombotic and subclinical arteriosclerosis biomarkers, and treatment in SLE patients with and without metabolic syndrome. Values are median (range) unless stated otherwise.
SLE patients with and without MetS undergoing treatment
More SLE patients with MetS took antihypertensive agents than those without MetS (p = 0.047). The rest of the treatments administered were similar in both groups (Table 2). The percentage of immunosuppressive agents taken in each group (with and without MetS, respectively) was as follows: azathioprine 4% versus 6%; cyclophosphamide 1% versus 1%; methrotexate 8% versus 8%; mycophenolate mofetil 18% versus 20%; and cyclosporine 0% versus 2%.
Differences in demographic, metabolic, and SLE-related factors between SLE patients with normal PWV and those with increased PWV
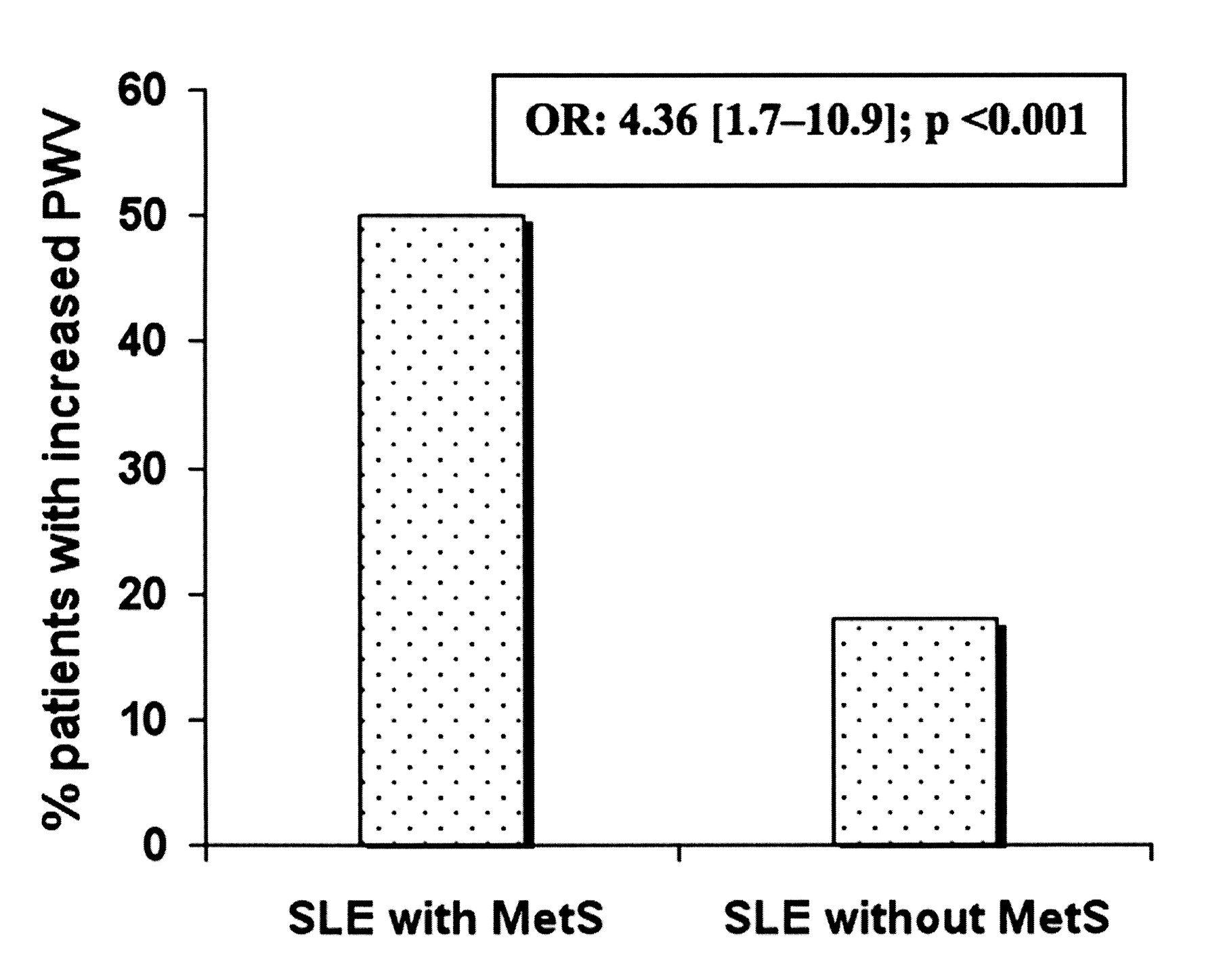
MetS was closely associated with increased PWV (50% vs 18% normal; OR 4.36, 95% CI 1.7–10.9, p < 0.001; Figure 1), and as expected MetS was associated with increased IR (48% vs 19% normal; OR 4.05, 95% CI 1.5–10.4, p = 0.002). The association between increased IR and increased PWV was no longer significant (p = 0.5) and the HOMA index was similar between patients with normal and those with increased PWV (Table 3). The main differences between patients with increased and normal PWV are shown in Table 3. To summarize, no differences were found in the variables related to lupus activity; however, some factors linked to ASCVD and atherosclerosis burden were more significant in the group with increased vascular stiffness. When evaluating treatment, it is notable that in the univariate analysis, the probability of use of HCQ tended to be higher in the SLE group with normal PWV, but this did not reach statistical significance (p = 0.056). Finally, patients with increased vascular stiffness had a significantly higher SDI.

{kind=link}
Percentage of SLE patients with increased pulse wave velocity (PWV) according to metabolic syndrome (MetS) status.
Characteristics of SLE patients with normal or increased pulse wave velocity (PWV). Values are median (range) unless stated otherwise.
In a multivariate analysis, age, male sex, presence of MetS, duration of SLE, and CRP levels were independently associated with an increased PWV (Table 4). This model correctly classified 71% of patients, with a cutoff value of 0.5.
Variables associated with increased pulse wave velocity in patients with SLE, using logistic regression.
DISCUSSION
The main finding of our study was a close link between the presence of MetS and increased aortic stiffness (OR 4.36, p < 0.001) and CRP levels in patients with SLE. These results support the hypothesis that MetS may contribute to the development of atherosclerosis in SLE patients, which could in part explain the excess of ASCVD observed in this population.
MetS occurs more frequently in SLE patients than in healthy subjects with similar characteristics5–7. Several studies have consistently shown an association between MetS and arterial stiffness13, which has been proven to be a marker of early vascular changes that may lead to major vascular disease8. Increased aortic PWV has been observed in SLE patients and even in adolescents11. Selzer, et al found that higher aortic stiffness in women with SLE was associated with a combination of SLE-related and CV risk factors24. Bjarnegrad, et al found that aortic PWV was positively associated with CRP and C3 in middle-aged women with SLE10. Finally, a link between MetS and carotid artery intima-media thickness has been found in patients with rheumatoid arthritis (RA)25. However, the influence of MetS itself on arterial stiffness in SLE patients remains largely unknown. Although initially a positive association between increased aortic stiffness and MetS in SLE patients was expected, the deleterious effect of MetS on arterial stiffness could equally be completely or partially overshadowed by SLE-related factors, in particular by low-grade systemic inflammation and therapies. In a recent study in which RA was accompanied by increased arterial stiffness, a reduction of systemic inflammation using anti-tumor necrosis factor-α therapies decreased aortic stiffness to a level comparable to that of healthy individuals26.
SLE and atherosclerosis share some biochemical mediators as a result of the underlying chronic inflammation status in both conditions. CRP and IL-6 have been associated with atherosclerosis burden24,27, MetS7,28, arterial stiffness10,29, and lupus disease activity30. In contrast, increased plasma concentrations of IL-8 and IL-10 have been found to correlate mainly with disease activity in SLE patients30,31. Thus, Asanuma, et al found no link between IL-8 and coronary artery calcification27. In our study, SLE patients with MetS had significantly higher levels of CRP and IL-6 compared to those without MetS. These data might be interpreted as the result of increased systemic inflammation due to major lupus activity. However, all measures associated with lupus activity, including SLEDAI, ESR, IL-8, IL-10, hemoglobin levels, white blood cell count, prednisone dose, and use of immunosuppressive agents, were similar in both groups. In contrast, lupus patients with MetS had higher levels of some new markers associated with ASCVD and MetS in SLE patients or in the general population, such as C37,9,10, uric acid7,32, homocysteine levels33–35, fibrinogen36–39, and D-dimer concentrations39,40. Consequently, it seems reasonable to attribute the excess of CRP and IL-6 levels to major atherosclerosis burden in the MetS group, as it coincides with the increased arterial stiffness observed in these patients. It is worth emphasizing that a recent study showed that IL-6 and CRP levels correlated with arterial stiffness in patients with SLE and RA28. On the other hand, MetS was associated with increased PWV in the univariate analysis (OR 4.36, p < 0.001; Figure 1) and in the multivariate model (Table 4). Moreover, SLE patients with increased PWV had higher biomarker levels of atherosclerosis such as CRP, uric acid, homocysteine, and fibrinogen. They also had a significantly higher level of HbA1c, recently identified as a biomarker independently associated with MetS41. Similarly, the education level of SLE patients with increased aortic stiffness was lower, which has also been linked to a higher prevalence of MetS affecting patients with SLE7 and the general population42.
Our results were particularly interesting because, unlike findings from Selzer, et al24 showing that increased aortic PWV was associated with a combination of SLE-related variables and traditional CV risk factors in the logistic regression analysis, we found that arterial stiffness was fundamentally associated with variables unrelated to SLE (age, presence of MetS, sex, and CRP levels), with the exception of the duration of lupus (Table 4). This discrepancy could be due to the differences in the demographic characteristics of patients included in the 2 studies.
Finally, increased PWV was associated with a higher SDI. This finding could be attributed to at least 2 facts: first, patients with increased arterial stiffness were older, and second, the duration of lupus in this group was significantly longer.
Regarding IR, this is thought to be a relevant contributor to the increased CV risk attributed to MetS in the general population. Indeed, IR contributed to the association between MetS and coronary artery calcification in nondiabetic subjects, independent of age, non-MetS risk factors, and CRP43. As expected, MetS was found to be associated with increased IR in SLE patients (OR 4.05, p = 0.002). However, the association between increased IR and increased PWV was not significant (p = 0.5). These results coincide with those obtained by Chung, et al44 in a recent study in which IR was associated with coronary artery calcification in RA, but not in SLE. The reason that increased PWV is associated with MetS, but not with IR, might be that, although closely linked, the 2 concepts are not exactly the same. It is well established that not all patients with MetS defined by the ATP III criteria have IR and not all patients with IR meet the criteria for MetS45; therefore, it is likely that patients included in both groups (MetS and IR) were not the same. On the other hand, in the study by Chung, et al the major contributing factors to IR in RA were inflammation markers and disease activity44. In contrast, in SLE, IR was associated fundamentally with obesity, but not with inflammation markers or lupus activity, except ESR44. In accord with these results, increased IR in our SLE patients was closely associated with obesity (OR 3.6, 95% CI 1.5–8.7, p = 0.003), CRP, ESR, and IL-6 levels, with SLEDAI scores being similar in patients with and without increased IR (data not shown).
Age could be a potential confounder in this study. The prevalence of MetS increases with age42. Yet advancing age, among other factors, is a major contributor to the development of sustained increased arterial stiffness46. SLE patients with MetS were significantly older than those without. Similarly, SLE patients with increased PWV were also older compared to those with normal PWV. In the multivariate analysis, age, as well as MetS, was independently associated with aortic stiffness. In the general population cohort, MetS accelerated the age-related progression of arterial stiffness with respect to subjects with 0, 1, or 2 CV risk factors, contributing to the development of premature vascular senescence in these patients13.
We found that therapies did not influence the results. Only antihypertensive agents were taken more frequently by SLE patients with MetS. Even so, these patients had higher PWV despite the fact that the most powerful method of treatment for reducing arterial stiffness is to vigorously treat HTN. It is worth noting that in the univariate analysis (but not in the multivariate analysis), non-use of HCQ tended to be associated with an increased PWV (p = 0.056). Selzer, et al9 found a significant association between the non-use of HCQ and increased PWV among premenopausal women. Similar results were also obtained by Tanay, et al47. Previously, Roman, et al found that HCQ treatment was associated with a lower presence of carotid plaque in SLE patients48. These findings suggest that HCQ might exert a protective effect on the vessel wall. We previously found that the use of HCQ was inversely associated with the presence of MetS in SLE patients7. Although the prevalence of MetS in SLE patients receiving HCQ (65%) was 15% lower than in those who did not take HCQ (76%), this inverse association was not statistically significant in the present study, probably due to the relatively small number of patients.
Some major limitations of our study should be considered. First, we did not include a healthy control group. Second, the design constituted a limitation, although this is common to the majority of studies that investigate underlying mechanisms of accelerated atherosclerosis in SLE. Since atherosclerosis is a slow process that evolves over months or years, a cross-sectional study based on single random measurements of aortic PWV and other inflammatory biomarkers cannot establish a cause-effect relation between MetS and vascular stiffness. For example, this design does not account for key issues such as how long a patient has had MetS. Therefore, prospective studies are needed to determine the exact role of MetS in the development of accelerated atherosclerosis in patients with SLE.
Despite these limitations, the results together suggest a close link between MetS and vascular stiffness in SLE. Moreover, MetS may increase aortic stiffness to a greater extent than IR and SLE activity. This aspect could be relevant in clinical practice, since MetS can be modified with appropriate pharmacological interventions and certain changes to lifestyle, which could prevent or delay the development of accelerated atherosclerosis in these patients. This hypothesis requires confirmation through further interventional studies.
Acknowledgments
We thank Ana Rosales for her invaluable assistance in organizing the clinical records. We also thank all patients for their cooperation and interest in our study.
APPENDIX.
Terms used in the text.
- Obesity
- body mass index ≥ 30 kg/m2.Hypertension, systolic blood pressure (SBP) ≥ 140 mm Hg or diastolic blood pressure (DBP) ≥ 90 mm Hg, or on antihypertensive therapy at the time of the study17.
- Pulse pressure
- difference between SBP and DBP.
- Diabetes mellitus
- on treatment with oral hypoglycemic agents or insulin, or fasting blood glucose (FBG) > 126 mg/dl at time of assessment18.
- Dyslipemia
- total cholesterol ≥ 190 mg/dl or low density lipoprotein ≥ 115 mg/dl, or high density lipoprotein (HDL) ≤ 40 mg/dl in men and ≤ 46 mg/dl in women or triglycerides (TG) ≥ 150 mg/dl, on treatment with hypolipemic drug therapy19.
- Smoking habit
- smoker: current smoking; nonsmoker: the remainder of the patients.
- Alcohol consumption
- nondrinkers: < 10 g ethanol/day; drinkers ≥ 10 g ethanol/day.
- Sedentary lifestyle
- < 200 minutes/week of moderate intensity physical activity, besides habitual activity.
- Family history of atherosclerotic cardiovascular diseases
- first-degree relative who had had a myocardial infarction or stroke < 55 years old in men, < 65 years old in women.
- Metabolic syndrome (National Cholesterol Education Program Adult Treatment Panel III definition)
- ≥ 3 of the following criteria: (1) waist circumference ≥ 102 cm in men, ≥ 88 cm in women; (2) SBP ≥ 130 mm Hg, or DBP ≥ 85 mm Hg, or use of antihypertensive therapy; (3) FBG ≥ 110 mg/dl; (4) triglycerides ≥ 150 mg/dl; (5) HDL < 40 mg/dl in men, < 50 mg/dl in women.
Footnotes
- Accepted for publication May 2, 2009.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.