

Abstract
Background. Pain in inflammatory arthritis (IA) is common and often multifactorial, and many different pharmacotherapeutic agents are routinely used for pain management. There are concerns that some current pain pharmacotherapies may increase the risk of adverse events in patients with concurrent cardiovascular (CV) or renal disease.
Methods. A systematic literature review was performed searching Medline, Embase, Cochrane Central Register of Controlled Trials, DARE, and Cochrane Database of Systematic Reviews. We also hand-searched conference proceedings for the American College of Rheumatology and the European League Against Rheumatism for 2008–2009.
Results. Our search identified 4782 studies, of which 190 were included for detailed review, but none met the inclusion criteria for our review. We identified 1 study of etoricoxib and diclofenac in non-IA populations [osteoarthritis (OA) or mixed OA and rheumatoid arthritis]. In that study, the presence of CV disease increased the likelihood of a further CV event 3-fold. Patients with 2 or more CV risk factors showed a 2-fold increased likelihood of adverse CV events.
Conclusion. Our review has highlighted a lack of specific evidence to guide clinicians in the management of pain in patients with IA and coexistent CV or renal disease. In the absence of this evidence, we suggest clinicians use nonsteroidal antiinflammatory drugs (NSAID) with caution in patients with preexisting CV disease or ≥ 2 CV risk factors. There is currently no evidence to advise clinicians considering other pain pharmacotherapies in the context of CV comorbidities. Current guidelines regarding the use of NSAID and opioids in moderate to severe renal impairment should also be applied to the IA population.
- PAIN
- RHEUMATOID ARTHRITIS
- ANKYLOSING SPONDYLITIS
- PSORIATIC ARTHRITIS
- SYSTEMATIC REVIEW
- CARDIOVASCULAR
- RENAL
This article is part of the 3e (Evidence, Expertise, Exchange) Initiative on Pain Management by Pharmacotherapy in Inflammatory Arthritis. The objective of our report was to systematically review the literature concerning one of the 10 selected questions as an evidence base for generating the recommendations1. This article is a modified version of a Cochrane Review that is specifically focused on rheumatoid arthritis (RA)2. The study protocol detailing the methods used to undertake the Cochrane review was published in January 20113.
The question was: “How do cardiovascular and renal comorbidities influence the choice of pain treatment in inflammatory arthritides?”.
Background
The inflammatory arthritides (IA) are a group of chronic, inflammatory, rheumatic diseases that primarily include RA, ankylosing spondylitis (AS), psoriatic arthritis (PsA), and other spondyloarthritis. They are characterized by pain, joint destruction, and subsequent loss of function4. Despite advances in the treatment of IA over the last decade, many patients continue to experience significant pain. Even in patients with relatively controlled disease, more than three-quarters reported regular moderate to severe pain5.
A range of drugs acting in a variety of ways (e.g., anti-inflammatory, analgesic) are commonly used to provide pain relief in IA, some of which have been shown to be associated with an increased risk of cardiovascular (CV) and renal adverse events. This was first highlighted by the withdrawal of rofecoxib [a cyclooxygenase 2 (COX-2) inhibitor] from the market due to an increased risk of myocardial infarction6. Subsequently several selective and nonselective nonsteroidal antiinflammatory drugs (NSAID) have been shown to be associated with an increased risk of cardiovascular disease (CVD)7.
The risk associated with pain pharmacotherapies is a particular concern as some forms of IA have themselves been shown to increase the risk of cardiovascular and renal adverse events. This has been best demonstrated in RA, where patients are known to have a reduced life expectancy, largely due to CVD. This is probably due to an increase in both traditional risk factors for atherosclerosis and the presence of chronic inflammation8,9,10.
At present clinicians must balance the patient’s need for effective pain control with the risks associated with prescribed pain medications. The aim of our review was to determine whether the safety and efficacy of pain pharmacotherapies for RA differ between those with and those without coexisting CV and/or renal disease, and to quantify the degree to which the presence of these comorbidities should modify clinicians’ choice of pain relief medications.
METHODS
Our review was carried out according to guidelines for systematic literature reviews as outlined by the Cochrane Collaboration. Before commencing the review a protocol3 was written and then followed during the review process.
Rephrasing the research question
The original clinical question was reformulated into an epidemiological research question according to the PICO (Patient, Intervention, Comparator, Outcome) method11. Patients were defined as adults with a diagnosis of RA, PsA, AS, or spondyloarthritis as defined by the study authors. In addition these patients had to have defined CV or renal disease prior to commencing the study. The interventions of interest were any drug used in clinical trials for pain relief as defined by the other review authors. For this review the comparator group was to be patients with IA treated with the same intervention but without CV or renal comorbidity. The major outcomes of interest were safety (number of withdrawals due to adverse events) and efficacy (patients reporting pain relief ≥ 30%). Minor outcomes were functional impairment and quality of life. We aimed to assess these outcomes in the short term (1–6 weeks), intermediate term (6–12 weeks), and long term (> 12 weeks) followup.
Search
We performed a systematic literature search for articles published between January 1950 and May 2010 via Medline, Embase, the Cochrane Central Register of Controlled Trials, the Cochrane Database of Systematic Reviews, and the Database of Abstract or Review and Effects. We also hand-searched conference proceedings from 2008–2009 from the American College of Rheumatology and European League Against Rheumatism (EULAR). In addition we searched websites of several regulatory agencies for adverse event reporting in the population of interest.
Selection of articles
We followed the methods recommended by the NHS Centre for Reviews and Dissemination12. Two reviewers (JM and AC) independently assessed each title and abstract for potential relevance to the review. Full articles were retrieved for included papers and for those articles where the title and abstract did not contain sufficient information to make an assessment. Articles that did not fulfil all the inclusion criteria were excluded from the systematic review.
Data extraction and quality appraisal
Both reviewers (JM and AC) independently reviewed the full articles, extracting data to standardized forms that included the prespecified quality appraisal. Randomized controlled trials (RCT) would be assessed using risk of bias13; controlled before-and-after trials (CBA) would be assessed using criteria outlined by the Cochrane Effective Practice and Organisation of Care group14; and cohort studies would be assessed for quality using the Newcastle-Ottawa Scale15. Authors were contacted to provide additional information if required.
Data analysis
For RCT we aimed to plot the results as point estimates, i.e., relative risks (RR) with corresponding 95% confidence intervals (95% CI) for dichotomous outcomes. For continuous data, results would be analyzed as mean differences (MD) and 95% CI between the intervention and comparator group. When different scales are used to measure the same outcome (e.g., level of pain) then standardized mean differences would be calculated instead.
We planned to report adverse events in each study descriptively, with studies grouped by design (RCT, CBA, intention-to-treat studies, cohort, case-control, and case series). For adverse events reported in CBA, cohort studies, and case series, frequency and RR of the event and time to event would be reported when data were available. For case-control studies, frequency of the event in cases and controls and the odds ratio (OR) would be reported. For data extracted from case series, the frequency of each event would be reported.
RESULTS
A total of 4782 articles were identified by our search strategy from which 190 articles were selected for more detailed review (Figure 1). The identified articles were predominantly related to NSAID and COX-2, and all but one of these studies assessed pain pharmacotherapy in patients with RA. None of the 190 reviewed articles met the inclusion criteria defined by our review. The majority of studies were excluded for 1 of 3 reasons: the study population was not exclusively IA and did not report outcomes for the IA subgroups separately; studies explicitly excluded patients with the comorbid conditions of interest; or data were reported in a way that did not allow comparison between patients with and those without the comorbidities of interest. For details of the PICO search strategy and reasons for exclusion of individual studies see the online Appendix available from www.3epain.com.
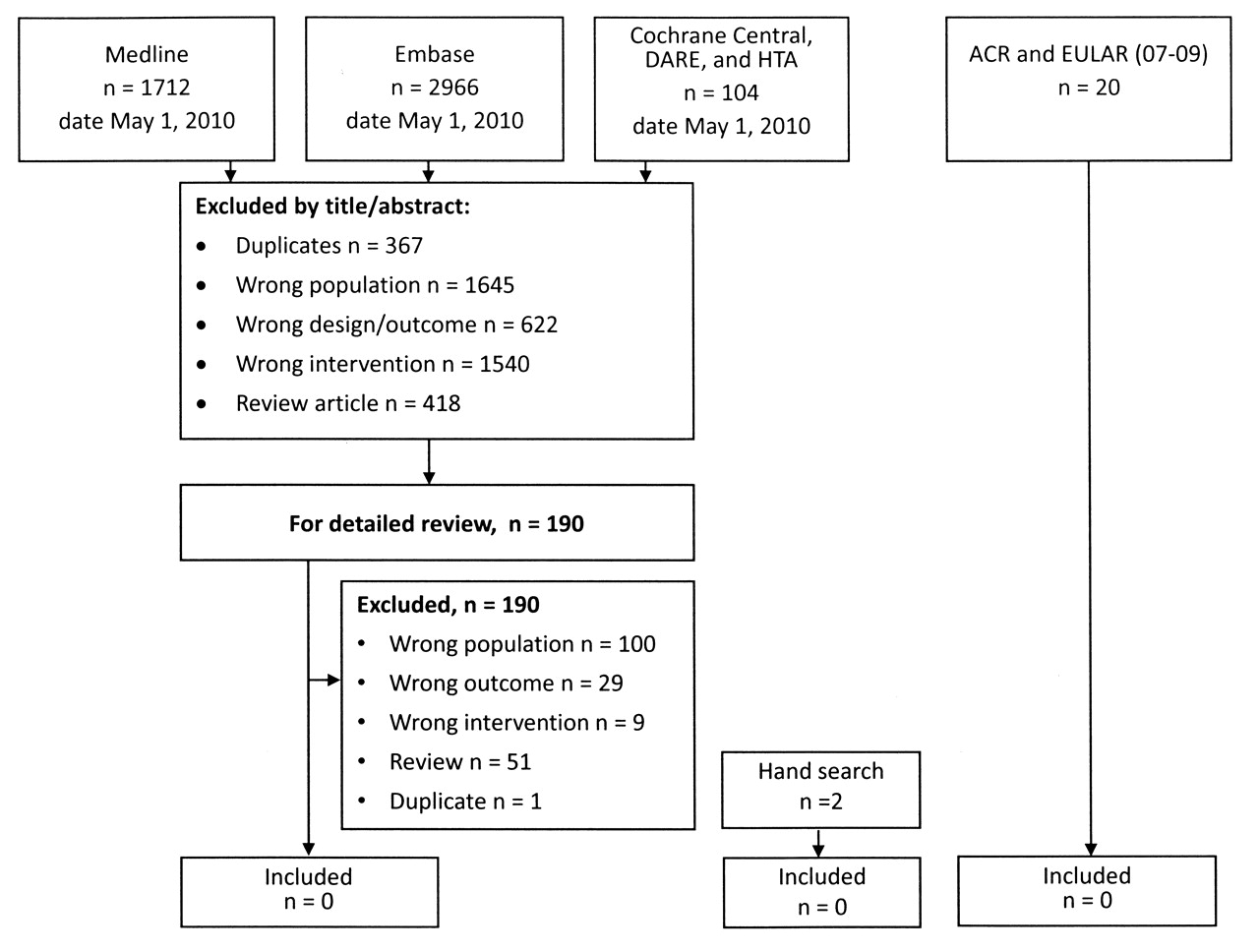
Literature search from which 190 articles were selected for detailed review. None of the articles met the inclusion criteria.
DISCUSSION
Our systematic review showed that there is no specific published evidence at the present time to advise clinicians considering pain pharmacotherapies for patients with IA and concurrent CV or renal disease. Our review is limited by a lack of available data. There have been several systematic reviews and metaanalyses demonstrating increased CV risk associated with NSAID use16,17. This effect appears to exist for all COX-2 and COX-1 inhibitors with the exception of high-dose naproxen, which does not appear to confer the same risk. Metaanalysis indicates that naproxen is risk-neutral when compared to placebo18.
Unfortunately, the published data included in these reviews tended to come from trials where the predominant disease population has not been IA. Further, many of the trials of NSAID excluded patients with CV or renal comorbidities, so there is a paucity of evidence to guide clinicians managing patients with these conditions. There is evidence in mixed populations (including both OA and IA) that the presence of CV comorbidities increases the likelihood of adverse CV events. The MEDAL program was a series of longterm multinational RCT [Multinational Etoricoxib and Diclofenac Arthritis Longterm (MEDAL) study; EDGE I; EDGE II] aiming to identify adverse events. In total 34,701 patients were recruited (24,913 with OA and 9787 with RA) and followed up for an average of 18 months. Data from the MEDAL program19 have shown that patients with established CV disease, treated with either etoricoxib or diclofenac, showed a 3-fold increased risk of experiencing an adverse CV event. Patients with 2 or more CV risk factors showed a 2-fold increased likelihood of adverse CV events.
In the absence of specific evidence in RA, current EULAR guidelines20 have advised that NSAID should be used with caution in the general RA population and have highlighted the increased need for caution in patients with CV risk factors or established disease. It is difficult to assess the safety of pain pharmacotherapies other than NSAID in mixed populations (including patients with IA) because preexisting CV and renal comorbidities were either rarely reported, or patients with these concurrent illnesses were excluded from the trial.
In conclusion, given the absence of specific evidence to guide clinicians when making decisions about pain management in IA with comorbid CV or renal disease, we advise caution when prescribing NSAID to patients with established CV risk factors, and extreme caution in patients with established CV disease. While no data were available for IA, it is likely that caution is also required if renal comorbidity is present. This conclusion was incorporated into the final recommendations of the 3e Initiative for the management of pain by pharmacotherapy in inflammatory arthritides1.
Footnotes
-
Based on a Cochrane Review published in the Cochrane Database of Systematic Reviews (CDSR) 2011, Issue 1, doi:10.1002/14651858.CD008952 (for details see www.thecochranelibrary.com). Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback, and the CDSR should be consulted for the most recent version of the review.








{kind=link}