

Abstract
Objective. To identify the significance of serum cartilage oligomeric matrix protein (COMP), a marker of cartilage turnover, in patients with early-stage rheumatoid arthritis (RA) in relation to other serologic variables and magnetic resonance imaging (MRI) features.
Methods. Ninety-eight patients with early-stage RA, whose disease duration from onset was less than 2 years, were enrolled. The objective measures at baseline were Disease Activity Score (DAS28), serum C-reactive protein (CRP), serum matrix metalloproteinase-3 (MMP-3), serum antibodies against cyclic citrullinated peptide (anti-CCP), and MRI features of both wrist and finger joints. The MRI features included the number of sites scored positive for synovitis, bone edema, and bone erosion.
Results. Serum COMP concentration was not different among groups identified with low, moderate, and high DAS28-CRP values. However, COMP values were statistically high in subjects positive for bone erosions on MRI compared with the subjects who were negative for bone erosions. A positive correlation of COMP with CRP and with MMP-3 values was also identified.
Conclusion. Elevation of COMP may reflect joint damage that is dependent on the synovial inflammatory process in early-stage RA.
- EARLY-STAGE RHEUMATOID ARTHRITIS
- CARTILAGE OLIGOMERIC MATRIX PROTEIN
- C-REACTIVE PROTEIN
- MATRIX METALLOPROTEINASE-3
- BONE EROSION
- MAGNETIC RESONANCE IMAGING
- ANTI-CYCLIC CITRULLINATED PEPTIDE ANTIBODIES
Synovitis in the context of rheumatoid arthritis (RA) leads to pathologic changes in adjacent structures, such as the articular cartilage, the cortical bone surfaces, and the underlying bone marrow, changes that have recently been verified by comparison of magnetic resonance images (MRI) on the day before surgery and the tissue specimens at joint replacement surgery (metacarpophalangeal or proximal interphalangeal joints) in patients with established RA1. These findings were obtained in patients with late-stage RA. A similar process should be occurring in early-stage RA, but it is very difficult to prove, since joint replacement surgery is performed infrequently in cases of early-stage RA. In contrast, qualifying pathologic features in the rheumatoid inflammatory process by serologic variables and MRI is recommended in early-stage patients rather than late-stage patients, since there may be fewer secondary disease process-independent phenomena in early-stage patients. We recently reported that MRI-proven synovitis, bone edema, and bone erosion in the wrist and finger joints in early-stage RA reflect systemic inflammatory indices of serum C-reactive protein (CRP) and serum matrix metalloproteinase-3 (MMP-3)2.
An interesting serum biomarker is cartilage oligomeric matrix protein (COMP), which is thought to be increased in the serum early in the course of RA as a sign of cartilage involvement3. However, it is difficult to identify early cartilage involvement by radiography, even in MRI. Thus, the estimation of early cartilage involvement in early-stage RA using established variables, including COMP, would be valuable for prognostication. Our study is the first report to qualify serum COMP values in patients with early-stage RA, in conjunction with other inflammatory indices, as well as MRI detection of early joint damage.
MATERIALS AND METHODS
Ninety-eight patients with early stage RA were enrolled from the Early Arthritis Clinic at the Unit of Translational Medicine, Department of Immunology and Rheumatology (First Department of Internal Medicine), Graduate School of Biomedical Sciences, Nagasaki University. They gave their informed consent to the protocol, which was approved by the Institutional Review Board of Nagasaki University.
The mean disease duration from onset of symptoms to entry was 4.9 months. Disease duration for each of the 98 patients was < 2 years, similar to other recent reports3,4. Baseline characteristics of the 98 patients are described in Table 1. All patients fulfilled the 1987 criteria of the American College of Rheumatology for RA5. Since serum COMP is reported to be high in patients with osteoarthritis (OA) of large joints6,7, we excluded the cases complicated with OA of hip or knee joint, classified according to the established criteria8,9.
Baseline characteristics of the 98 patients with early-stage RA.
The following variables were examined at entry. Serologic tests included COMP (COMP ELISA®, AnaMar Medical AB, Göteborg, Sweden), CRP (Eiken Chemical Co. Ltd., Tokyo, Japan), MMP-3 (Daiichi Pure Chemicals, Fukuoka, Japan), and anti-CCP antibodies (Diastat Anti-CCP, Axis-Shield, Dundee, UK; cutoff value 4.5 U/ml). Clinical disease activity was qualified by the Disease Activity Score (DAS28-CRP; high disease activity > 4.1, low disease activity < 2.7, remission < 2.3)10. MR images of both wrists and finger joints (1.5 Tesla Sigma device; GE Medical Systems, Milwaukee, WI, USA) were evaluated for bone edema, bone erosion, and synovitis in 15 sites in each finger and wrist, i.e., the distal radioulnar joint, radiocarpal joint, mid-carpal joint, first carpometacarpal joint, second–fifth carpometacarpal joint (together), and first–fifth metacarpophalangeal joints (proximal interphalangeal joints) separately (a total of 30 sites in both hands), as we reported2,11,12. The MR images were interpreted independently by 2 board certified radiologists experienced in musculoskeletal imaging (MU and ST), who were blinded to the clinical status of the patients. Both radiologists read each image according to the definition, as described13,14, and disagreements were resolved by consensus. The degree of MRI features was evaluated as we recently published: synovitis; the number of sites scored as positive for MRI synovitis, bone edema; number of bones scored positive for bone edema, bone erosion; and number of bones scored positive for MRI bone erosion2.
Serum COMP concentration, in general, is reported to be elevated with age3, as we found in the 98 patients with early-stage RA we examined (r = 0.39, p < 0.001). Thus, a partial correlation coefficient adjusting for age was calculated. Since MMP-3 was not normally distributed, we conducted logarithmic transformation. Differences between groups were examined using the age-adjusted mean. A test for trend was performed using the general linear modeling method. A p value < 0.05 denoted the presence of a statistically significant difference.
RESULTS
Table 1 shows the baseline characteristics of the 98 patients. Briefly, the median DAS28-CRP at entry was 4.3. Forty-seven percent of subjects were positive for MRI-proven bone edema, and 33% were positive for bone erosions. The median serum COMP at entry was 10.3 U/ml, median titer of anti-CCP antibodies was 20.3 U/ml, and seropositivity to anti-CCP antibodies was found in 66% of subjects. For MMP-3, the median serum concentration was 66.6 ng/ml, and seropositivity for MMP-3, denoted as in the higher than normal range, was 42%. As described3, a positive correlation was found between serum COMP value and age in the 98 patients (r = 0.39, p < 0.001, Spearman’s rank correlation test), and thus a partial correlation coefficient adjusting for age was calculated in the following data, as described above.
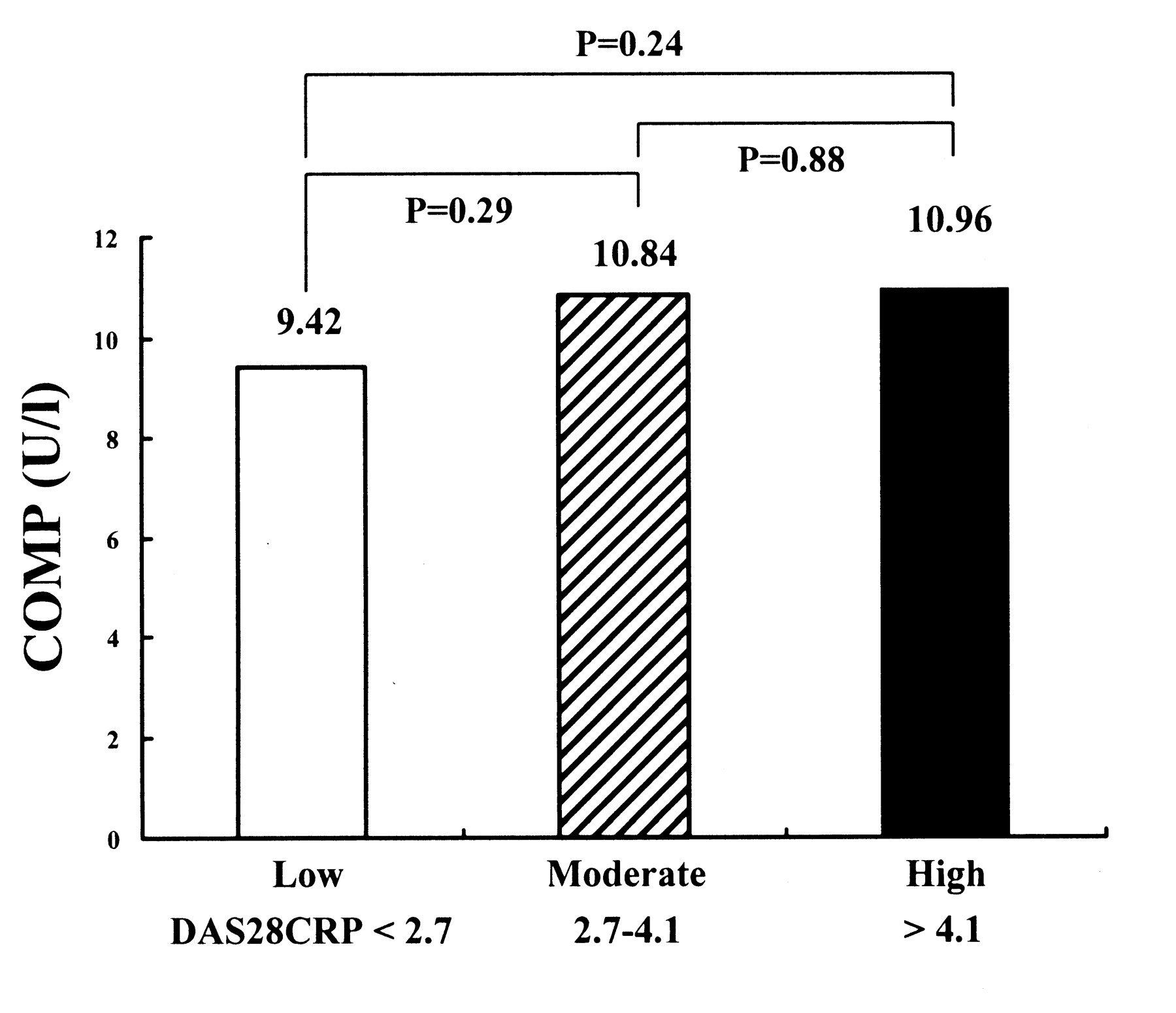
A partial correlation coefficient adjusting for age showed positive correlation of COMP with CRP (r = 0.21, p = 0.035) as well as MMP-3 values (r = 0.20, p = 0.046). Although the difference was not statistically significant, a weak association was determined between the number of MRI-proven bone erosions and the serum COMP (r = 0.19, p = 0.06). Therefore, we divided the 98 patients into 2 groups according to the MRI-proven bone erosions, and examined the distribution of serum COMP. Figure 1 shows that the age-adjusted mean concentration of serum COMP was statistically significantly high in the subjects who were positive for bone erosions on MRI, compared with subjects who were negative for erosions. As suspected, the mean values of CRP and MMP-3 were also high in the subjects who were positive for bone erosions on MRI (data not shown). We also examined the distribution of serum COMP by DAS28-CRP, and observed no differences among subjects who had low, moderate, and high DAS28-CRP scores (Figure 2). A test for trend showed no association between serum COMP and DAS28-CRP (p = 0.31). In addition, the age-adjusted mean concentration of serum COMP was not statistically different between subjects with different anti-CCP antibody status (mean COMP concentration was 10.54 U/l in subjects who were anti-CCP antibody-positive; and 11.26 U/l in subjects who were anti-CCP antibody-negative; p = 0.36).
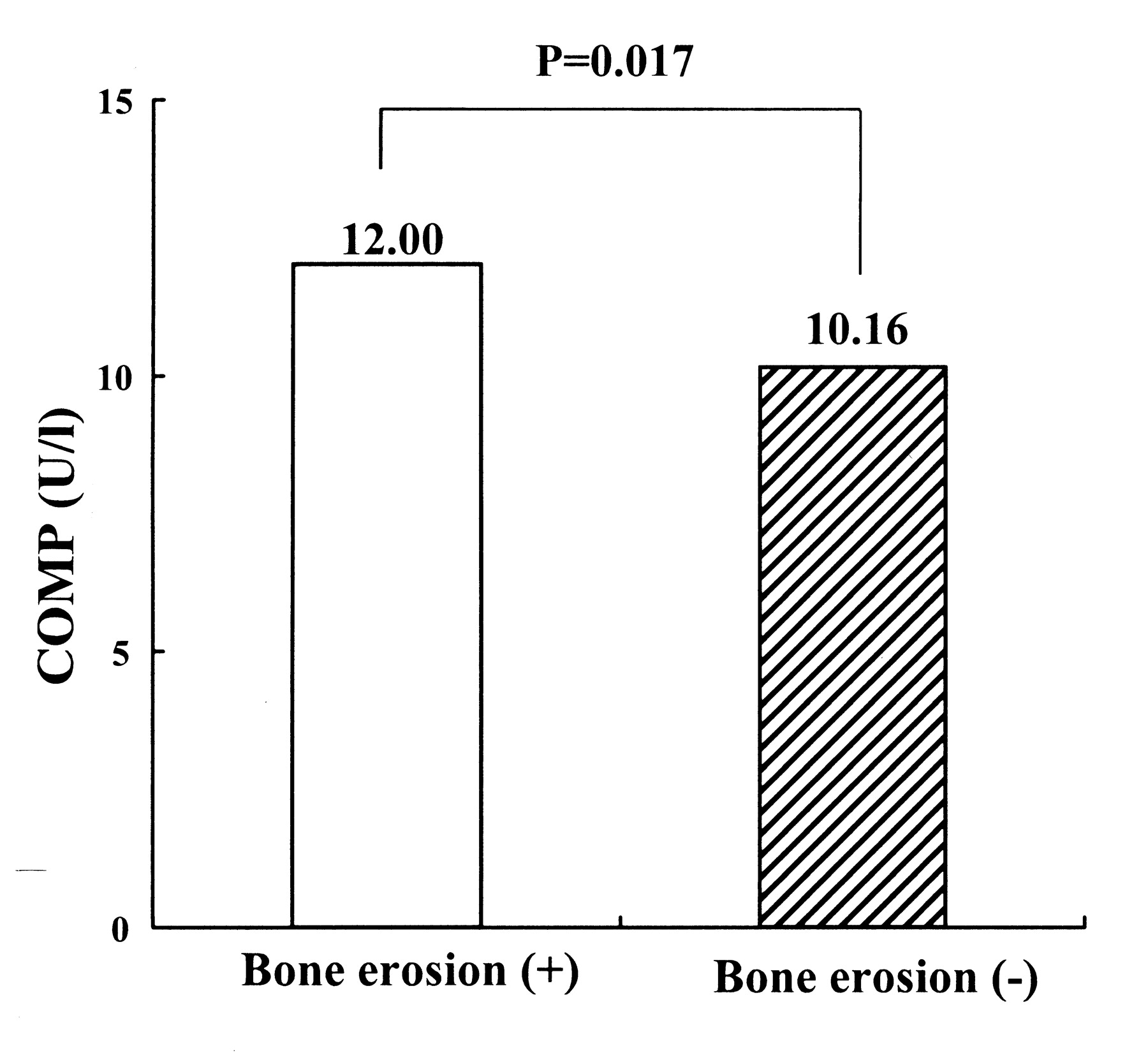
The age-adjusted mean serum COMP concentration was high in subjects with MRI-proven bone erosions (n = 32) compared to those without bone erosions (n = 66).

Serum COMP values of 98 patients with early-stage RA were not different among those with low, moderate, and high scores for DAS28-CRP. P value between the groups was calculated by age-adjusted mean. P value was nonsignificant.
DISCUSSION
COMP is a marker of articular cartilage damage, originally described as the determinant of radiographic progression in OA of the large joints, such as hip OA and knee OA6,7,15. Recently, serum COMP was evaluated in patients with RA, and was found to be preferentially elevated not in late-stage RA but in early-stage RA3. In addition, high serum COMP at baseline in early-stage RA indicates future radiographic progression3. The serum COMP concentration at baseline may also reflect the therapeutic efficacy of radiography in patients with active RA: low COMP at baseline predicted a better radiographic outcome in clinical trials of adalimumab treatment in RA16. We have investigated the role of serologic variables as well as MRI features of the wrist and fingers in early-stage RA2,11,12; in the present study we focused on the serum COMP value. MR images of the small joints in the wrist and fingers were closely examined, and thus patients with early-stage RA with clinically definite large-joint OA (hip and knee OA) were excluded, since a large amount of COMP could be produced from the affected articular cartilage, which might weaken the significance of the RA-related COMP value.
We initially expected COMP values to correlate with bone damage-prone markers, such as MMP-3, and MRI-proven bone edema and erosion. Raw data also showed an association of COMP with the number of MRI-proven bone erosions (r = 0.33, p = 0.02); however, age-adjusted data identified statistically significant association of COMP with only CRP and MMP-3. Since rheumatoid bone and cartilage damage are suggested to be driven by the neighboring synovial tissues1, it was recognized that the inflammatory index provided by CRP and MMP-3 correlates with the cartilage turnover marker COMP. In addition, the findings that COMP concentrations were higher in the subjects with MRI-proven bone erosions than in those without erosions may support the speculation that rheumatoid synovial inflammation promotes articular cartilage turnover in situ in early-stage RA. Our findings that CRP and MMP-3 levels were high in the subjects with MRI-proven bone erosions also support this. Our recent study showed that MRI-proven bone edema, in early-stage RA, was significantly correlated with inflammatory indexes and DAS2, but in the present study we did not see a relationship between the serum COMP value and MRI-proven bone edema. These observations may indicate that COMP reflects another aspect of the disease process of RA, which should be confirmed by our continuing prospective study.
This is the first report to investigate the significance of the relation of serum COMP value with MRI detection of early joint damage in early-stage RA. Serum COMP values at entry correlated with CRP and MMP-3 values, and MRI-proven bone erosion also predicted high serum COMP concentrations in study subjects.
Footnotes
-
Supported by a grant from The Ministry of Health, Labour and Welfare, Japan.
- Accepted for publication December 3, 2008.








{kind=link}
{kind=link}