

Abstract
Objective. To describe the treatment profile of multimorbid patients with rheumatoid arthritis (RA) in contrast to patients with RA only.
Methods. COMORA (Comorbidities in Rheumatoid Arthritis) is a cross-sectional, international study assessing morbidities, outcomes, and treatment of patients with RA. Patients were grouped according to their multimorbidity profile assessed by a counted multimorbidity index (cMMI). Treatment for RA was categorized as use of biologic disease-modifying antirheumatic drugs (bDMARD), in particular tumor necrosis factor inhibitors (TNFi), synthetic DMARD (sDMARD) use only, nonsteroidal antiinflammatory drug (NSAID) use, and corticosteroid use. Logistic regression models were performed to determine the OR of bDMARD, TNFi, sDMARD, NSAID, or corticosteroid use based on a patient’s cMMI and global region after adjusting for age, disease activity, disease duration, educational level, and previous DMARD therapy.
Results. Out of 3920 patients, 32.7% received bDMARD; 59.9% sDMARD only, 51.1% used concomitant NSAID, and 54.8% used corticosteroid. Regional differences were observed with the most frequent use of bDMARD in the United States (46.5%) and lowest in North Africa (9%). After adjusting for confounders in logistic regression, the OR for bDMARD use was reduced for each additional morbidity (OR 0.89, 95% CI 0.83–0.96). Similar results were found for TNFi (OR 0.91, 95% CI 0.84–0.99), whereas the OR for use of sDMARD was increased (1.13, 95% CI 1.05–1.22). No significant change of OR was found for NSAID or corticosteroid use.
Conclusion. In this study, the odds of bDMARD use decreases 11% for each additional chronic morbid condition after adjustment for regional differences, disease activity, and other covariates.
Because inflammatory rheumatic conditions are mostly systemic diseases, a high prevalence of coexisting disorders can be observed. The average patient with rheumatoid arthritis (RA) has 1.6 additional conditions, increasing with age, disease duration, and/or disease activity1,2. While these are mostly considered as comorbidities in the setting of an index disease, in chronic morbid patients, multimorbidity might be a more useful concept. In contrast to the concept of comorbidity, it uses a patient-centered approach, rather than focusing on a single index condition3. Multimorbidity takes into account all potential interactions of coexisting diseases and its effect on patients’ overall well-being.
It is known from previous studies that multimorbid patients with RA are potentially undertreated for their concomitant diseases4, which reduces important outcomes of these ailments. However, because of multimorbidity, one may also observe less intensive treatment of RA than indicated5. This might be partly a consequence of older age and general tendency to undertreat elderly patients6,7. It might also be because of concerns of increased adverse events or interaction with other medications in the presence of multimorbidity8. This can cause higher activity of RA and therefore impairs all its major outcomes, such as physical function, quality of life, work productivity, or even mortality. Research has shown that there is no difference in treatment response in elderly patients with RA (65 yrs and older) compared with younger patients9,10. Nevertheless, coexisting diseases have been identified as negative predictors for response to therapy11,12; therefore, multimorbid patients with RA might require more intensive treatment to achieve treatment targets. Treatment recommendations such as treat-to-target aim for optimal therapeutic approaches to achieve remission, considering the presence of coexisting morbidities13.
Previous studies have shown a negative association of biological disease-modifying antirheumatic drug (bDMARD) initiation and presence of comorbidity in patients with RA5, investigating only small cohorts without incorporating the concept of multimorbidity. To our knowledge, this is the first large international study to assess the cross-sectional treatment profile of multimorbid patients with RA from 17 different countries worldwide. Our aim was to assess the effect of multimorbidity on treatment status, accounting for factors that affect treatment decisions, including disease activity and regional differences.
MATERIALS AND METHODS
Study cohort
Comorbidities in Rheumatoid Arthritis (COMORA) is an international, cross-sectional, observational study of more than 3900 patients with RA recruited in 17 countries worldwide between 2011 and 201214. The National Principal Investigators were instructed to recruit rheumatologists representative of their respective countries to conduct the study. Consecutive patients visiting participating rheumatologists were included if they were 18 years or older and fulfilled the 1987 American College of Rheumatology (ACR) classification criteria for RA15. Ethical approval was obtained by all local institutional review boards or ethics committees.
Assessment of multimorbidity
In COMORA, variables of disease activity and severity, as well as information on specific morbidities, were collected by each participating rheumatologist using charts, medical records, and/or patient interview (for details see original COMORA paper14). Based on these data, we calculated the counted multimorbidity index (cMMI), an index based on the effect of multimorbidity on health-related quality of life (HRQOL) that originally included 40 different morbid conditions16. cMMI was developed and validated in a large RA cohort, in which it was shown to perform better in explaining the effect of comorbidity on HRQOL than the commonly used Charlson Comorbidity Index. Out of 40 conditions, 12 conditions were reported in COMORA (hypertension, obesity, depression, cancer, asthma, coronary heart disease, viral hepatitis, chronic obstructive pulmonary disease, diabetes mellitus, chronic kidney disease, diverticulitis, and stroke), and cMMI was calculated by enumerating the particular number of morbidities for each patient. As shown in a previous work, a short form of the index including only 12 conditions served as a valid alternative16. Patients were divided into 5 groups according to cMMI: RA only (cMMI = 1) and multimorbid RA with 1 (cMMI = 2), 2 (cMMI = 3), 3 (cMMI = 4), and 4 or more (cMMI ≥ 5) additional chronic morbid conditions.
Outcome of interest
To assess treatment patterns, we used information on current and previous RA therapy collected in COMORA: DMARD [type, starting and/or ending date, and reason for discontinuation of all synthetic DMARD (sDMARD) and bDMARD ever used], nonsteroidal antiinflammatory drug (NSAID; current intake collected according to the Assessment of Spondyloarthritis international Society recommendations, including name and dosage)17, and corticosteroids (intake in mg/day as well as the estimated total intake of corticosteroids from the beginning of the disease). We categorized information on RA treatment: current use of sDMARD only (yes/no), current use of bDMARD in general (yes/no), current use of tumor necrosis factor inhibitor in particular (TNFi; yes/no), current corticosteroid intake (yes/no), current NSAID intake (yes/no), and number of previous DMARD (synthetic and/or biologic).
Statistical analyses
We categorized patients according to cMMI into 5 groups and compared patients’ characteristics across the groups. In the primary analyses, we assessed whether certain treatment patterns may be associated with the multimorbidity status. In unadjusted analyses, we investigated differences of current and previous treatment status between groups of patients with different cMMI using the chi-square test and ANOVA testing for linear trend. We also looked for regional differences and split the cohort into region of origin: (1) Europe: Austria, France, Germany, Hungary, Italy, the Netherlands, Spain, and UK; (2) United States; (3) Asia: Japan, Korea, and Taiwan; (4) Latin America: Argentina, Uruguay, and Venezuela; and (5) North Africa: Egypt and Morocco.
In adjusted analyses, we included factors associated with RA treatment, such as disease activity by Clinical Disease Activity Index (CDAI), disease duration, age, sex, education level, serological status, number of previous DMARD, and region. We decided a priori on clinically meaningful variables to be included in logistic regression analyses. In 4 different models we calculated the odds of current treatment with bDMARD, TNFi, sDMARD, NSAID, or corticosteroids for different status of multimorbidity according to cMMI. Using the Box-Tidwell test, we could confirm that including cMMI as a continuous variable in regression models did not violate assumption of linearity. In secondary analyses, we calculated OR of bDMARD and TNFi use for specific morbid conditions.
All statistical analyses were carried out using IBM SPSS Statistics version 21.
RESULTS
The study sample consisted of 3920 patients, and 2563 (65.4%) were multimorbid with more than 1 chronic condition in addition to RA. The median cMMI was 2 (25th/75th percentile 1/3, range 1–10). Patients’ characteristics of the total study sample as well as subgroups of patients according to their cMMI are shown in Table 1, with significant differences between RA only and multimorbid patients with RA. In general, multimorbid patients were older and experienced higher disease activity measured by CDAI and Disease Activity Score at 28 joints, worse physical function evaluated by Health Assessment Questionnaire (HAQ) or modified HAQ, and longer disease duration compared with patients with RA only. This decrease of physical function and quality of life with increasing cMMI, and the increase in disease duration, age, and disease activity with increasing cMMI follows a linear trend (Table 1). The prevalence of different morbid conditions is shown in Supplementary Table 1, available online at jrheum.org.
Patients’ characteristics for the total study sample (first column) as well as subgroups of patients according to their level of the cMMI. Values are mean (SD) or % unless otherwise specified.
Unadjusted analyses
Overall, 92.6% of the patients were receiving DMARD therapy, 32.7% received a bDMARD, 59.9% were receiving sDMARD only, 51.1% had concomitant NSAID use, and 54.8% corticosteroid intake. In unadjusted analyses, there were no differences in frequency of current DMARD use, TNFi use, or corticosteroid use between RA only and multimorbid patients with RA (p > 0.05). In contrast to adjusted analyses, without adjusting for important confounders, higher rates of bDMARD use in multimorbid patients with RA were observed. The frequency of current NSAID use was significantly lower in multimorbid patients (Supplementary Table 2, available online at jrheum.org).
To account for regional differences, data from different countries were grouped according to their geographical region. In general, the United States had the highest median cMMI of 3 (range 1–10) compared with all other regions (Europe median 2, range 1–9; Asia median 2, range 1–6; Latin America median 2, range 1–7; North Africa median 2, range 1–6; Kruskal-Wallis test p < 0.01).
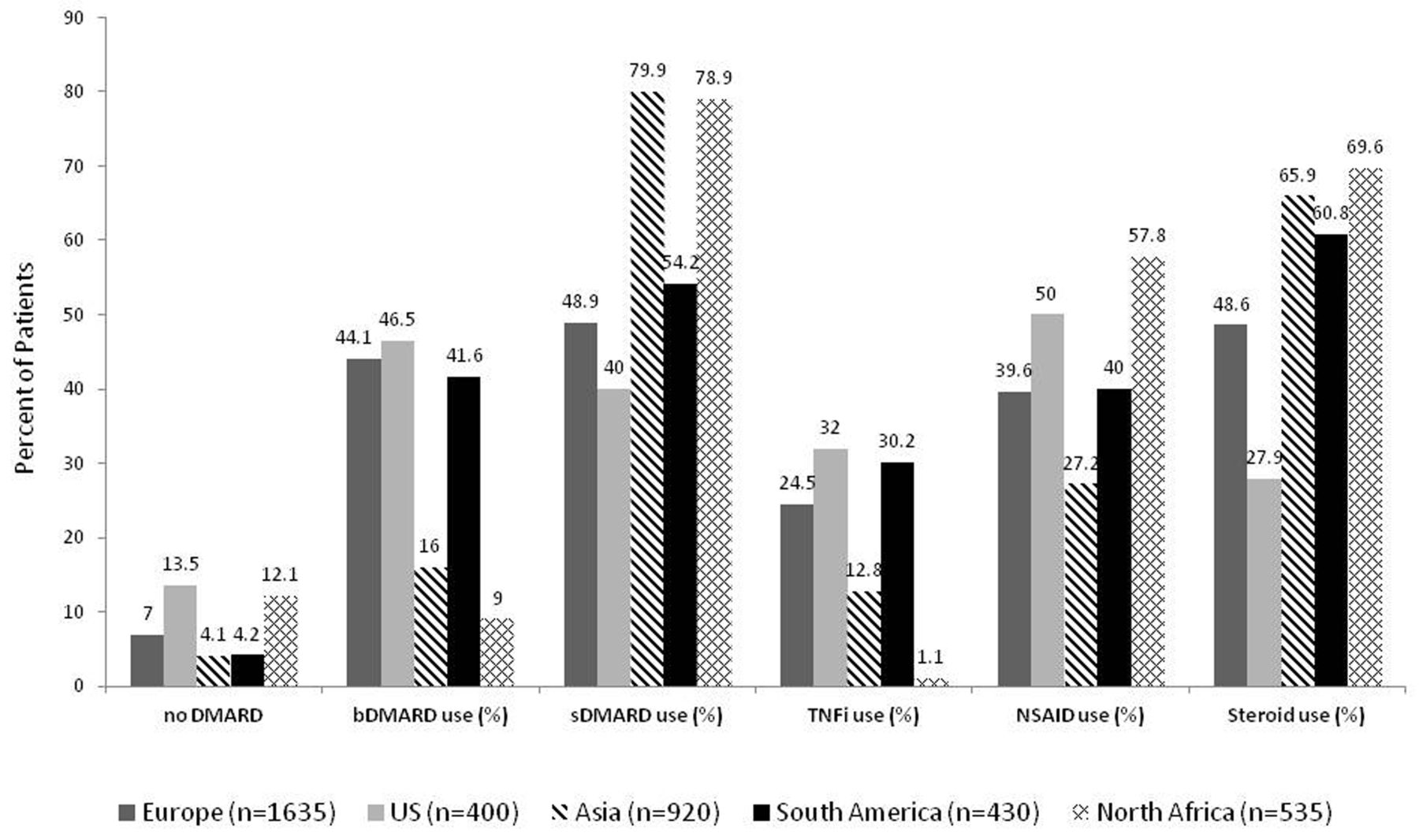
Looking at overall regional differences of current treatment use, we found significantly less bDMARD and TNFi treatment use in the North African (bDMARD 9%, TNFi 1.1%) and Asian (bDMARD 16%, TNFi 12.8%) subgroups of patients compared with all other regional subgroups (p < 0.01). The United States had the highest bDMARD use (46.5%) and the lowest corticosteroid use (27.9%; Figure 1). Regional differences across patients with different level of cMMI are displayed in Supplementary Figure 1, available online at jrheum.org.
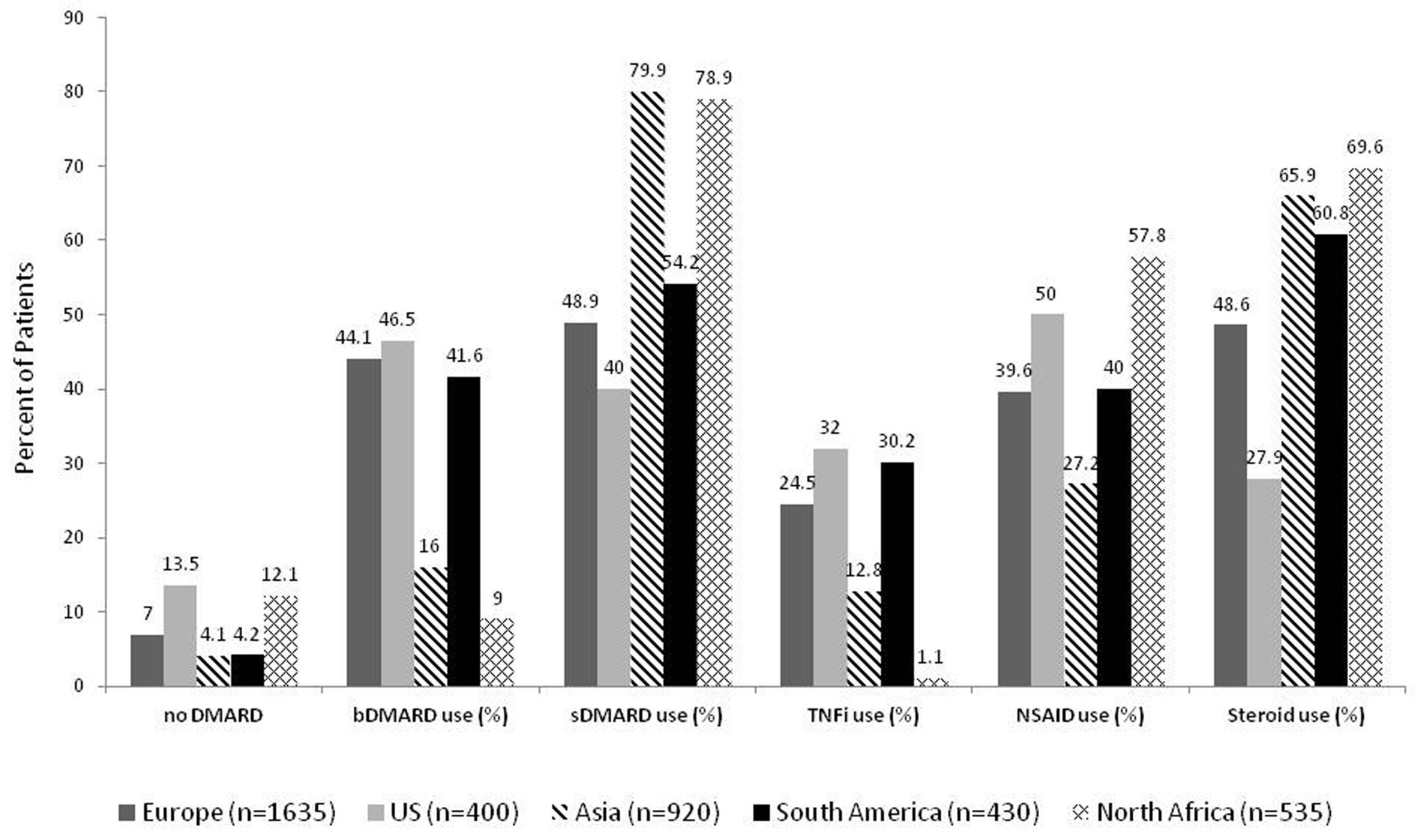
Regional differences of current treatment status including bDMARD, TNFi, sDMARD, NSAID, and corticosteroid (steroids) use. DMARD: disease-modifying antirheumatic drugs; bDMARD: biological DMARD; TNFi: tumor necrosis factor inhibitor; sDMARD: synthetic DMARD; NSAID: nonsteroidal antiinflammatory drug.
Adjusted analyses
In logistic regression analyses, we examined the use of (1) bDMARD, (2) TNFi, (3) sDMARD, (4) NSAID, and (5) corticosteroids as the outcome in relation to cMMI; models were adjusted for disease activity by CDAI, disease duration, age, sex, educational level, number of previous DMARD, serological status, and geographic region. Nagelkerke R2 was 0.26 for the model predicting current bDMARD use, 0.17 for current TNFi use, 0.25 for sDMARD use only, 0.14 for current NSAID use, and 0.14 for current corticosteroid use. In the final model, the OR of current bDMARD use for cMMI was 0.89 (95% CI 0.83–0.96, p = 0.05), which means that for each point increase of cMMI, the odds of current bDMARD use decreases by 11%. Similar results were found for TNFi use: OR cMMI = 0.91 (95% CI 0.84–0.99, p = 0.04; Table 2). Further, Asia or North Africa had a significantly lower OR of receiving either bDMARD or TNFi compared with Europe. The OR for sDMARD use only was 1.13 (95% CI 1.05–1.22, p = 0.003). The OR of current NSAID or corticosteroid use was not significant for cMMI.
Multivariate logistic regression models predicting the probability of current bDMARD use, TNFi use, sDMARD use only, NSAID use, and corticosteroid use (steroids). Variables included in the model are the cMMI, age, disease duration, number of previous DMARD, disease activity, education level, and region. For bDMARD and TNFi, the OR is decreasing with increasing value of the cMMI. Values are OR (95% CI).
In secondary analyses, we calculated OR for each morbid condition, showing significant lower OR of bDMARD use and TNFi use for cancer (OR 0.67, 95% CI 0.49–0.90; Supplementary Table 3, available online at jrheum.org). OR was also lower for other conditions, though not statistically significant. To ensure that our primary results were not driven by the presence of cancer, we repeated the logistic regression models explained above, excluding patients with cancer and found very similar OR (results not shown).
DISCUSSION
We were interested in the treatment profile of multimorbid patients with RA compared with patients with RA only. In a large international cohort, we found that the OR of being treated with a bDMARD in general or a TNFi in particular was lower for multimorbid patients, with a decrease of roughly 10% per additional morbid condition. This would mean that patients with a high number of chronic conditions in addition to RA were less likely to receive a biological agent, even if it might be necessary because of high RA disease activity despite synthetic DMARD treatment. Further, the OR for sDMARD use only increased, probably reflecting rheumatologists’ greater comfort of using these agents in patients with a greater multimorbidity burden.
Even though these are cross-sectional analyses, findings are consistent with previous studies, showing that the initiation of biological therapy is less likely in patients with RA with concomitant diseases5. This might be a consequence of older age and a general tendency to undertreat elderly patients6,7, but also attributable to concerns of increased adverse events or polypharmacy8. Current treatment recommendations of the ACR, the European League Against Rheumatism, or the treat-to-target task force13,18,19 aim for optimal therapeutic outcomes, considering concomitant diseases.
Optimal treatment of RA affects the patient’s overall condition. Concomitant chronic conditions, such as cardiovascular disease, are closely linked to the inflammatory process of RA20,21,22. Intensive treatment that controls RA activity might improve insulin resistance and cardiovascular risk, which has been shown for TNFi23,24,25. Withholding bDMARD in multimorbid patients with RA might worsen the patient’s RA and other chronic conditions present. It might increase the incidence of concomitant diseases and worsen overall outcomes.
On the contrary, treatment with more potent agents such as bDMARD might increase the risk of serious adverse events, such as infections or malignancies26,27. Several drugs are contraindicated in patients with specific morbidities (for example, abatacept in chronic obstructive pulmonary disease28,29, TNFi in recent-onset cancer30, etc.) that makes treatment of multimorbid patients with RA more challenging.
After adjusting for important covariates, we confirmed the negative association of multimorbidity and bDMARD use reported in literature. We used a described multimorbidity index that allows for easy assessment of the patient’s overall disease status. Moreover, in contrast to previous studies, we used a large international RA cohort of more than 3900 patients from various regions and with varying disease activity and disease duration. COMORA included patients from 17 different nations, allowing us to also compare current treatment across different global regions. We could observe regional differences of bDMARD and TNFi use, with highest overall use in the United States and lowest use in North Africa. Because TNFi are one of the most commonly used bDMARD in the treatment of RA, and contraindications differ from those of other biological agents, we specifically addressed the association of TNFi use and multimorbidity in separate analyses.
We found significantly lower odds of bDMARD/TNFi use if cancer was present. For other morbidities (such as stroke, chronic kidney disease, etc.), we found similar results, though not statistically significant; this might be because of the low prevalence of the diseases in our cohort or the fact that some conditions (such as hypertension or obesity) were regarded as rather mild and presumably would not influence treatment choices when treating patients with RA.
Several limitations need to be addressed. COMORA is a cross-sectional study. Therefore, it is not possible to investigate causality; mitigated treatment might be because of multimorbidity or vice versa. Second, as mentioned in the original COMORA paper14, the study population might not be fully representative for all patients with RA in the participating countries. Despite the efforts to recruit rheumatologists working in different practice settings to enroll patients, the study does not include patients with RA from general practices not seeing a rheumatologist. This might reflect a selection bias as patients seeing a rheumatologist might experience more severe disease activity. Further, even though COMORA has no specific inclusion or exclusion criteria except for having RA, there might be a selection bias, recruiting only those patients doing well or being more compliant. There might be some inter-country variability, especially for bDMARD therapy, explained by different country-specific treatment guidelines, number of approved bDMARD, reimbursement policies, and more31. Across the 5 regions, there could be cultural differences as well as differences in affordability, accessibility, and acceptability of DMARD therapy. Nevertheless, the large sample of patients enrolled from each country allows accounting for some of the limitations. Finally, even after adjusting for all important covariates, our models explained only up to 25% of the reason for using bDMARD. Several factors that might affect the prescription of bDMARD, such as patient preferences, insurance status, or patient income, were not evaluated in COMORA and therefore not included in our model.
We were able to show that multimorbid patients with RA were less likely to receive bDMARD or TNFi therapy compared with patients with RA only; there were also regional differences in bDMARD use. Even though these are cross-sectional findings with several caveats, we should be aware of potential undertreatment of patients with 1 or more additional chronic conditions than RA. Longitudinal studies are needed to investigate whether this undertreatment affects longterm outcomes such as disease activity, radiographic progression, physical function, organ damage, or mortality.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
The authors thank all patients and investigators who participated in our study.
Footnotes
The Comorbidities in Rheumatoid Arthritis study (COMORA) is conducted with the support of an unrestricted grant from Roche Ltd.
- Accepted for publication March 26, 2015.








{kind=link}