

Abstract
Objective. Telomeres protect against chromosomal end damage and shorten with each cell division; their length may be a marker of cardiovascular and overall biological aging. We examined the hypothesis that reduced telomere length is associated with increased coronary atherosclerosis in rheumatoid arthritis (RA).
Methods. We performed a cross-sectional study in 145 patients with RA and 87 control subjects frequency-matched for age, race, and sex. Coronary artery calcium score was determined by noncontrast cardiac computed tomography. Telomere length was measured from whole blood DNA, using real-time quantitative polymerase chain reaction and expressed as telomeric product to a single-copy gene product ratio (T/S ratio). Associations between telomere length, coronary artery calcium score, and 28-joint Disease Activity Score (DAS28) were assessed with Spearman correlation, proportional odds logistic regression, and linear regression, adjusting for age, race, and sex.
Results. Telomere length was significantly inversely correlated with age in patients with RA (ρ = −0.37, p < 0.001) and control subjects (ρ = −0.39, p = 0.001). Among patients with RA, for every interquartile range (IQR) decrease in telomere length (T/S ratio), the odds of higher coronary artery calcium score increased by 38% (95% CI: 4–60) after adjusting for age, race, and sex (p adjusted = 0.03). Telomere length was not associated with DAS28 (p adjusted = 0.17). Telomere length was not significantly different in patients with RA [median (IQR): 1.02 units (0.9–1.11)] compared to control subjects [1.05 units (0.95–1.17); p = 0.10].
Conclusion. Telomere length is inversely associated with coronary artery calcium score, independent of age, race, and sex in patients with RA.
Premature cardiovascular (CV) disease is the leading cause of early death in patients with rheumatoid arthritis (RA)1. Traditional risk factors such as age do not fully account for the increased risk observed in RA2. In many ways RA can be considered a disease of accelerated aging of both the immune and CV systems3,4. Thus, measures of biological aging, such as decreasing telomere length, may be altered in RA and better reflect CV age in these patients.
Telomeres are non-coding DNA sequences that cap the ends of chromosomes, protecting them from loss of DNA and from being recognized as double-strand breaks5. Telomeres shorten with every cell division, making them a form of biological clock6. Indeed, telomere length is believed to be a better marker of biological age than chronological age7,8,9, and thus may better estimate the risks of age-related diseases, such as CV disease. In fact, in many populations, short telomere length, independent of age, is associated with the presence and development of CV disease10,11,12,13.
Shortened telomeres have been found in several cell types of patients with RA14,15,16, but their association with CV disease has not been studied. We hypothesize that telomere length would be inversely associated with coronary atherosclerosis in patients with RA.
MATERIALS AND METHODS
Study population
This was a cross-sectional study of 145 patients with RA and 87 control subjects. These subjects are part of a cohort in which we have studied CV risk factors and coronary atherosclerosis2,17,18. Recruitment and study procedures have been described17. Subjects were 18 years of age or older and patients with RA met the American College of Rheumatology 1987 criteria for RA19. Patients with RA and control subjects were matched for age, race, and sex. Control subjects did not have a diagnosis of inflammatory disease. The study was approved by the Vanderbilt Institutional Review Board. All subjects gave written informed consent.
Study procedures
Clinical characteristics, laboratory measurements and coronary artery calcium scores were obtained as previously described2,17,18. Briefly, the 10-year CV risk was determined by the Framingham risk score20. Fasting lipid panels were performed in the hospital clinical laboratory. High sensitivity C-reactive protein (hsCRP) was measured by ELISA or the hospital clinical laboratory. Coronary artery calcium scores were determined by electron beam computed tomography and calculated in Agatston units21.
DNA extracted from whole blood was used to measure telomere length of peripheral blood leukocytes. Telomere length was determined with a quantitative PCR–based method by a reference laboratory (Telome Health Inc.)22,23. Telomere product (T) was compared to a single-copy gene product (S) in each sample, and this ratio was compared to that of a genomic DNA standard, creating a T/S ratio, which is proportional to the average telomere length22,23. Each sample was run in triplicate, standard reference DNA was run in quadruplicate, and 3 separate quality controls (mean T/S ratio range 0.78 to 2.26) were run in triplicate in each 384-well plate. The relative standard error for each sample was calculated. Samples with >12.5% relative standard error were re-assayed. The interassay coefficient of variation for this assay is 6.45%23.
Statistics
Based on 145 patients with RA and 87 control subjects and a T/S ratio SD of 0.19, we had 90% power to detect a difference as small as a T/S ratio of 0.08 or higher, which is less than half an SD in T/S ratio.
Descriptive statistics were calculated as median with interquartile range (IQR) for continuous variables, and frequency and proportions for categorical variables.
The independent association between telomere length and disease status (RA or control) was assessed with multivariable linear regression models, with adjustment for age, race, and sex. Additional analyses were performed only in the RA group. Spearman’s rank correlation coefficients (ρ) were calculated to assess the correlation between telomere length and continuous variables. Proportional odds logistic regression was used to assess association between telomere length and coronary artery calcium score as the outcome, with adjustment for age, race, and sex. Multivariable linear regression models were used to assess the association between telomere length and clinical and laboratory measures, with adjustment for age, race, and sex. Because age strongly influences telomere length and coronary artery calcification, age was included in models using restricted cubic splines to account for nonlinear effects24.
To assess whether the relationship between telomere length and coronary artery calcium score was modified by disease status, we used proportional odds models with independent variables including the cross-product term disease status (RA vs control) and telomere length with adjustment for age, race, and sex.
Triglyceride, hsCRP, and urinary F2-isoprostane concentrations were natural logarithm–transformed to improve normality of residuals. Statistical analyses were performed using R version 2.15.1 (www.r-project.org) and IBM SPSS Statistics v22. Two-sided p values ≤ 0.05 were considered statistically significant.
RESULTS
Clinical characteristics
Clinical characteristics of patients with RA (Table 1) have been reported17. The patients with RA were a median (IQR) age of 53 years (45–61), 88% white, 69% female, and the majority had moderate disease activity by 28-joint Disease Activity Score [DAS28; 3.85 units (2.57–4.75)].
Clinical characteristics of patients with rheumatoid arthritis. Continuous variables are presented as median (interquartile range). Categorical variables are presented as n (%).
Coronary artery calcium and telomere length in RA
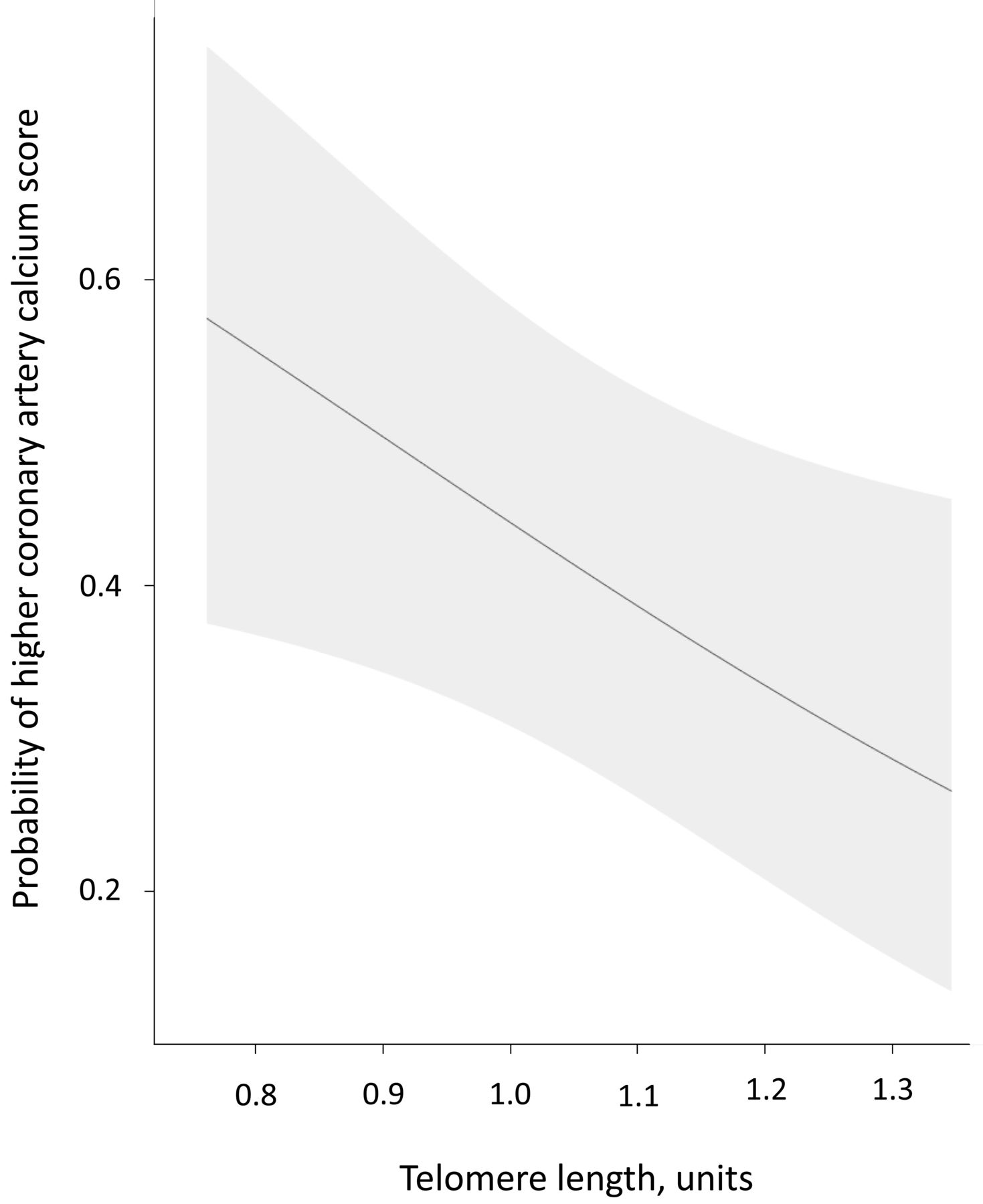
Telomere length was inversely correlated with coronary artery calcium score in univariate analysis (ρ = −0.37, p < 0.001) in patients with RA. After adjusting for age, race, and sex, the odds of higher coronary artery calcium score increased by 38% (95% CI: 4–60; p adjusted 0.03) for every IQR decrease in telomere length (T/S ratio; Figure 1).

Association between telomere length and coronary artery calcium score in patients with rheumatoid arthritis. The probability of higher coronary artery calcium score increased significantly with decreasing telomere length, independent of age, race, and sex (p = 0.03). The figure was adjusted to a 53-year-old white female. Shaded region represents the 95% CI.
CV risk factors and telomere length in RA
Age was inversely correlated with telomere length (ρ = −0.37, p < 0.001), as expected, as was Framingham risk score (ρ = −0.27, p = 0.001; Table 2; Supplementary Figure 1, available online at jrheum.org). The association between Framingham risk score and telomere length was no longer significant after adjustment for age, race, and sex (p adjusted = 0.63). Telomere length was similar in males [1.01 units (0.88–1.09)] and females [1.04 units (0.93, 1.12); p = 0.35], including after adjustment for age and race (p = 0.44). Lipid concentrations, including total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglycerides were not associated with telomere length in univariate or adjusted analyses (Table 2). Smoking history measured in pack-years was weakly inversely associated with telomere length (ρ = −0.16, p = 0.05, p adjusted = 0.07). Systolic blood pressure, diastolic blood pressure, and diagnosis of hypertension were not significantly associated with telomere length in univariate or adjusted analyses (all p > 0.05; Table 2).
Relationship between telomere length and cardiovascular risk factors in patients with rheumatoid arthritis.
Disease-related variables and telomere length
There were no significant relationships between telomere length and disease-related factors or inflammation (Table 3). The following characteristics were not significantly associated with telomere length: disease activity measured by DAS28 score, disease duration, positive rheumatoid factor, hsCRP, cumulative corticosteroid dose, and cumulative methotrexate dose (p > 0.05; Table 3). Similarly, there was no significant association between current medication use (methotrexate, leflunomide, hydroxychloroquine, anti-tumor necrosis factor-α agent, corticosteroids, and nonsteroidal antiinflammatory drugs) and telomere length (p > 0.05; Supplementary Table 1, available online at jrheum.org).
Relationship between telomere length and inflammation and rheumatoid arthritis disease-related factors.
Telomere length in RA vs controls
We compared telomere length among patients with RA to control subjects (n = 87) matched for age, race, and sex [age: 52 yrs (44–58); 84% white; 64% female]. Telomere length was not significantly different in patients with RA [1.02 units (0.9–1.11)] compared to control subjects [1.05 units (0.95–1.17); p = 0.10; Figure 2]. Based on the previously published relationship between T/S ratio and terminal restriction fragment (TRF) length in kilobases (kb; TRF in kb = 2.16*(T/S ratio) + 4.02)23, the median telomere length was about 6.223 kb in RA and 6.288 kb in control subjects. In control subjects, as was the case in patients with RA, telomere length was inversely associated with age (ρ = −0.39, p = 0.001). In control subjects, telomere length was not significantly inversely associated with coronary calcium score (ρ = −0.18, p = 0.10) or with adjustment for age, race, and sex (p = 0.25). Despite this difference between RA and control subjects, disease status did not significantly modify the association between telomere length and coronary calcium score by interaction analysis (p = 0.69).
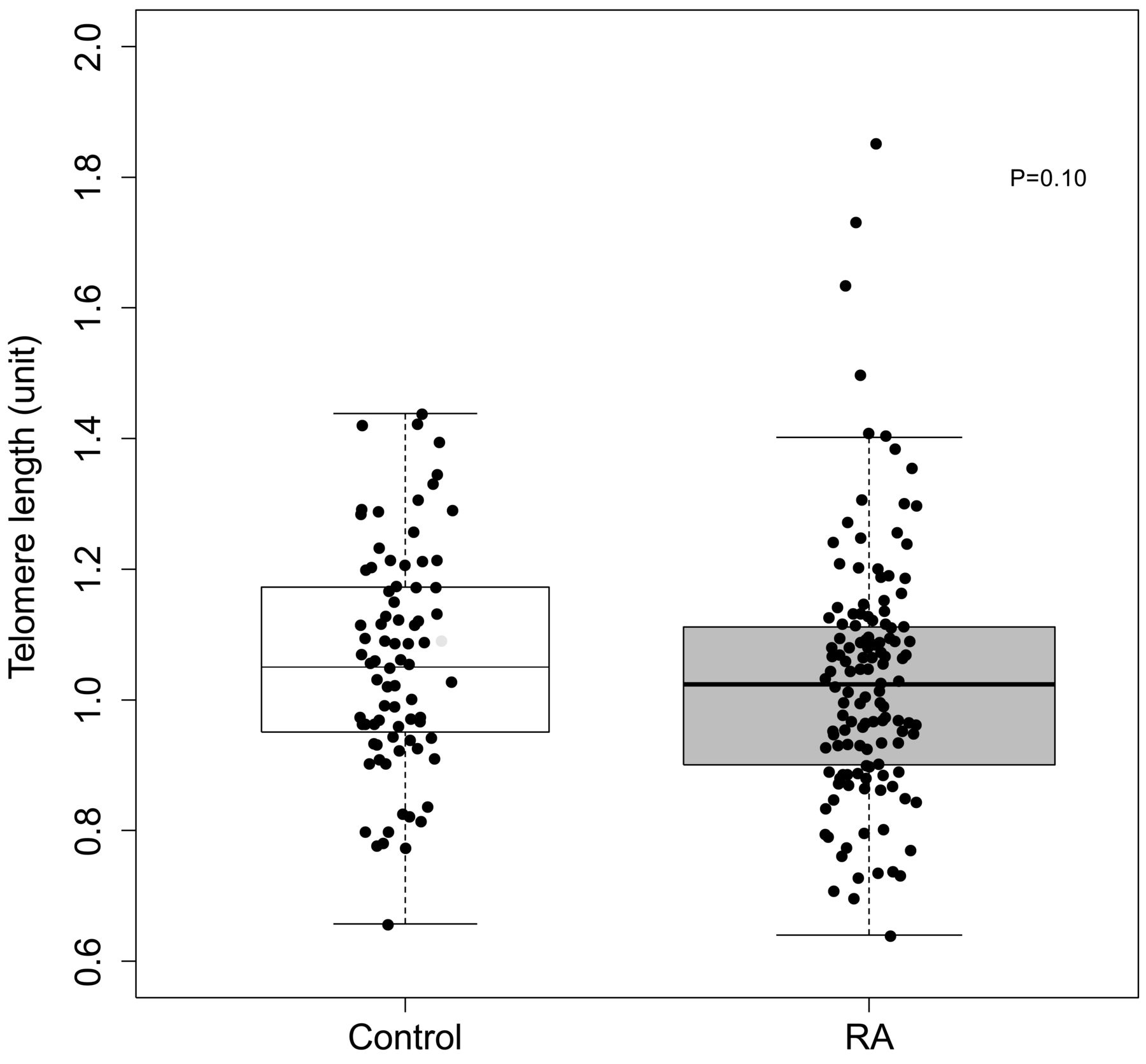
Telomere length in patients with rheumatoid arthritis (RA) and control subjects. Telomere length was not significantly different in patients with RA [n = 145; 1.02 units (0.9–1.11)] compared to control subjects [n = 87; 1.05 units (0.95–1.17), p = 0.10].
DISCUSSION
The major finding of our study is that telomere length is inversely associated with coronary artery calcium score independent of age, race, and sex in patients with RA. Telomere length is not significantly shorter in patients with RA compared to control subjects, matched for age, race, and sex, and is not associated with RA disease-related factors or CV risk factors.
Telomere length has been found to be shorter in patients with RA compared to control subjects in some cell populations such as naive CD4 T cells and CD34+ hematopoietic stem cells14,15,16. This is partially due to aberrant regulation of telomerase, an enzyme that elongates telomeres of some stem cells and other cells under highly proliferative conditions25. For example, stimulated naive CD4 T cells from patients with RA failed to upregulate telomerase, leading to shorter telomeres during clonal expansion14. Such telomerase deficiency, however, is not present in all RA cell populations. Indeed, memory T cells have similar telomerase activity and similar telomere length, comparing RA and control subjects16.
An intriguing observation in studies that evaluated telomere length in RA in specific cell populations14,15,16 or in peripheral leukocytes26 was that there was no significant relationship between telomere length and disease activity, inflammation, or disease duration. Our findings are consistent with those observations. Thus, it is likely that factors other than proliferative pressure from systemic inflammation drive telomere loss in some RA cell populations. Such factors may include impaired regulation of telomerase14, deficiency of other DNA repair enzymes27, and genetic factors26,28. Also, considering the reported association between atherosclerotic CV disease and shortened telomere length in other populations, this association in RA is of interest.
Others have also found that shorter leukocyte telomere length was significantly associated with more extensive coronary atherosclerosis measured by coronary artery calcification in non-RA populations, such as 325 subjects without diabetes, coronary heart disease, stroke, or cancer29, and a population-based sample of 250 urban Palestinians30. Shortened telomere length has also been associated with CV events in several patient populations, in both cross-sectional and prospective studies. For example, telomere length measured in peripheral blood leukocytes was significantly shorter in patients with premature myocardial infarction (n = 203) compared to age-matched control subjects (n = 180)12. Moreover, in a prospective study that included 19,383 participants followed for up to 19 years, the HR for myocardial infarction was 1.13 (95% CI: 1.04–1.23), independent of age and sex, for every 1000 base pair (bp) decrease in telomere length at baseline31.
Many suggest that telomere length is a better assessment of biological age than chronological age7,8, and this may explain its association with atherosclerotic CV disease, which can be viewed as premature aging of the vasculature9. RA is a disease associated with a prematurely aged immune system4 as well as premature atherosclerosis17. Indeed, coronary artery calcification has been viewed as a better indicator of vascular aging than chronological age32; thus, investigation of telomere length as an indicator of CV age in RA is of interest. We found that shorter telomere length was associated with higher coronary calcium score, independent of age, race, and sex. This finding may support the idea that, from a vascular perspective, telomere length is a better reflection of biological age than chronological age, or that shortened telomere length itself may be a driver of CV disease development. Conversely, shortened telomere length and coronary calcium may be common endpoints influenced by the same confounders; however, we did not find robust correlations between telomere length and CV risk factors. Regardless of pathway, shorter telomere length was associated with greater coronary atherosclerosis burden in patients with RA.
We found that telomere length in peripheral blood leukocytes was shorter, but not significantly so, in RA compared to matched control subjects. This contrasts with the finding of a prior study in which telomere length was shorter in 176 patients with RA compared to 1151 control subjects26. The previous study found a 0.31 kb difference between RA and control subjects, and we found about a 0.07 kb difference. Based on an expected decreased in telomere length of about 30–40 bp/year6, this would equate with a “biological age” difference between RA and control subjects of about 8–10 years in the previous study and about 2 years (though not significant) in our study. Differences in study design might explain these findings. In the prior study, although adjustments were made for age, the mean age of patients with RA was significantly higher than control subjects (63.8 compared to 48.2 yrs), and because age has the greatest influence on telomere length, this may have influenced those results. The previous study had a much larger control sample size; however, a posthoc calculation indicated that our study had 90% power to detect the equivalent of a 0.17 kb difference in telomere length between patients with RA and control subjects. Thus, we had sufficient power to detect the larger difference of 0.31 kb found by the prior study. It is possible, however, that the true difference in peripheral blood leukocyte telomere length comparing RA to control subjects is smaller than our study was powered to detect.
Our study has some limitations. Given the cross-sectional design, we could only show associations between telomere length and coronary calcium score and were unable to define the mechanisms underlying the observation. The telomere length was assessed in the whole blood, precluding examination of specific cell populations, and we did not examine structural changes of the telomeres in RA. Also, we did not evaluate change in telomere length over time, which may have an influence on biological and CV aging. The patients with RA had relatively well-controlled disease, so we are limited in the ability to define the relationship between severe active disease and coronary calcium score. We did not stratify by HLA-DRB1 status, which may contribute to shortened telomere length26,28.
Telomere length is inversely associated with coronary artery calcium score, independent of age, race, and sex in patients with RA, but is not significantly associated with other CV risk factors or disease activity.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Footnotes
Supported by grants: Arthritis Foundation Clinical to Research Transition Award, Rheumatology Research Foundation Innovative Research Award, US National Institutes of Health Grants P60 AR056116, T32 AR059039, KL2TR000446, K23 AR068443, and CTSA award UL1TR000445 from the US National Center for Advancing Translational Sciences. This report’s contents are solely the responsibility of the authors and do not necessarily represent official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
- Accepted for publication April 6, 2016.








{kind=link}
{kind=link}