

Abstract
Objective. We analyzed early mortality after total hip arthroplasty (THA) in patients with inflammatory arthritis (IA), adjusting for medical comorbidities and socioeconomic background.
Methods. Data on 6690 patients with IA who underwent THA during 1992–2012 were extracted from the Swedish Hip Arthroplasty Register. Data on comorbidity, measured using the Charlson Comorbidity Index (CCI), and socioeconomic data were gathered from the Swedish National Inpatient Register and Statistics Sweden. The CCI was divided into low (0), moderate (1–2), and high (> 2). Cox proportional hazards models were fitted to calculate adjusted HR of early mortality, with 95% CI.
Results. Twenty-five patients (0.4%) died within 0–90 days, giving a 90-day unadjusted survival rate of 99.6% (CI 99.5–99.8). Comorbidity was associated with an increased risk of death within 90 days postoperatively [high vs low CCI: adjusted HR 9.0 (CI 1.6–49.9)]. There was a trend toward lower risk of death during the period 1999–2005, although patients operated on during this period had more comorbidities than those operated on from 1992 to 1998. A large proportion of patients was re-admitted to hospital within 90 days after the index procedure (30.2%), but rarely for cardiovascular reasons.
Conclusion. Medical comorbidity and an age above 75 years are associated with a substantial increase in the risk of early death after THA in patients with IA. Awareness of potential risk factors may alert clinicians and thus improve perioperative care.
There is an overall trend toward a reduced incidence of orthopedic surgery in patients with inflammatory arthritis (IA)1. Nevertheless, this population constitutes a large proportion of all patients who undergo joint replacement surgery2. Patients with IA seem to have an increased risk of complications and early mortality following major joint arthroplasty when compared to patients with osteoarthritis (OA)3,4,5,6. Because the population with IA has a high burden of medical comorbidities, this increased risk would be expected.
However, there is no consensus on the notion of increased early mortality in total hip arthroplasty (THA) patients with IA. Several studies report that early mortality after THA or total knee arthroplasty in patients with IA is not higher than in patients with OA3,6,7.
Most studies of mortality after hip arthroplasty in patients with IA lack information on medical comorbidities and socioeconomic background variables3,4,6,7,8,9,10,11,12. Thus, the risk of death — adjusted for medical comorbidities and other confounding factors — after one of the major orthopedic treatment modalities in patients with IA remains unclear.
Therefore, the aim of our study was to analyze early mortality after THA in patients with IA, taking medical comorbidities and socioeconomic background variables into account. Medical comorbidity was assessed using the widely established Charlson Comorbidity Index13. Moreover, we intended to study whether there was a temporal trend toward reduced mortality rates during the last 2 decades.
MATERIALS AND METHODS
Source of data
In Sweden, all citizens have a personal identification number that is used in every contact with healthcare providers. Since 1992, the Swedish Hip Arthroplasty Register (SHAR) contains individualized data based on this personal identification number. We therefore extracted data on all patients with IA who had an elective primary THA between 1992 and 2012. The SHAR has been repeatedly validated. National coverage is complete, and completeness of registration has been stable at around 96%–98%14,15. We did not include patients operated on for hip fracture, metastatic disease, or with revision joint replacement. The unique personal identification number for any Swedish resident allowed linkage between the SHAR and the registers mentioned below. This in turn allowed access to information on medical comorbidities and socioeconomic background variables for all patients.
Data on medical comorbidities were obtained from the Swedish National Inpatient Register (IPR)16. The Charlson Comorbidity Index (CCI) was computed based on data obtained from the year preceding the index procedure but excluding the inpatient period during which the index procedure was performed13,17. The CCI includes several major disease categories such as cardiovascular (CV), cerebrovascular, chronic pulmonary, liver, renal, and gastrointestinal, along with diabetes, and solid and hematological tumors. Each category is weighted as 1, 2, 3, or 6 points, and the score is the sum of these weightings. The cases were classified into 3 levels of comorbidity: low (score 0), moderate (score 1–2), and high (score > 2)18. Socioeconomic factors, including level of education and household and personal income, were extracted from Statistics Sweden. The level of education was presented in 4 groups (none or < 9 yrs, 9 years, high school, and university), and income was divided into quarters. Age at index surgery was divided into 3 groups (< 60, 60–75, and > 75 yrs). Persons who died or emigrated during followup were identified through the Total Population Register.
Our primary endpoint was early (0–90 days and 91–180 days) mortality after the date of the index surgery (THA). Secondary endpoints were overall survival and readmissions due to CV reasons within the first 90 days after the index procedure. CV disease was defined as myocardial infarction, chronic heart failure, peripheral vascular disease, and/or cerebrovascular disease19.
Ethics
Ethical approval was granted by the Regional Ethical Review Board in Gothenburg (approval number: 2013/360–13). All individuals registered in the SHAR had received written information about the SHAR and were given the choice not to participate in the register or associated research. Written informed consent for participation was not obtained, consistent with the Swedish Patient Data Law of 2009.
Statistics
Followup started on the day of surgery and ended on the day of death, emigration, or censorship at December 31, 2012, whichever came first. Continuous data were described using means, SD, and ranges. To describe estimation uncertainty, 95% CI were used.
Kaplan-Meier survival analysis was performed to calculate unadjusted cumulative survival. Cox proportional hazard regression models were fitted for each covariate at a time to calculate crude HR with CI, and covariates were subsequently included in multiple regression models to calculate adjusted HR with CI. The choice of covariates included in multiple regression models was based upon assessment of relevance and noninterference using directed acyclical graphs. We checked the assumption of proportionality of hazards graphically and by calculating scaled Schoenfeld residuals.
The material was divided into 3 time periods (1992–1998, 1999–2005, and 2006–2012) to investigate temporal trends in the demography, comorbidity, surgical technique, and mortality in the investigated cohort.
Logistic regression analysis was used to investigate the CCI in the 3 time periods described above, adjusting for age, sex, diagnosis, level of education, and income. The low CCI score was defined as the reference level and compared with the moderate and the high CCI score. OR were calculated together with 95% CI. The level of significance was set at p < 0.05. All analyses were performed using the PASW statistics package version 18 (SPSS Inc.) and R software (version 3.0.2) together with the “rms” and “Gmisc” packages.
Characteristics of the study population
We identified 6690 patients with IA who underwent at least 1 THA during the study period from 1992 to 2012. Among these, 2013 patients received a contralateral THA at a later timepoint. In cases with bilateral THA, the insertion of the first THA was chosen as the index procedure. The proportion of females was 72% and the mean age at surgery was 63 years (range 12–92). Implant survival was 90.6% (95% CI 81.1–100%) after 9.5 years. The majority (78%) of the patients had rheumatoid arthritis (RA) as their primary diagnosis. The remaining patients had inflammatory joint conditions related to other unspecified, noninfectious arthritic conditions (14%), psoriatic arthritis (5%), and ankylosing spondylitis (3%). Most patients had a moderate CCI at surgery (72%). About half of the patient cohort had a 9-year education (Table 1).
Description of the study population. Data are n (%) unless otherwise indicated.
RESULTS
Temporal changes in the demography, medical comorbidity, and choice of surgical technique in patients with IA undergoing THA
The sex distribution was stable over the 3 investigated time periods, and there were no major differences in the distribution of patients over the 3 age groups (Supplementary Table 1, available online at jrheum.org). There was, however, an increase in the comorbidity burden in patients undergoing THA during 1999–2005 and 2006–2012 compared with 1992–1998. A moderate or a high degree of comorbidity was more common during the 2 later time periods when compared with the first period (Supplementary Table 2, available online at jrheum.org). This observation remained true also after adjustment for age, sex, diagnosis, level of education, and income (Figure 1).
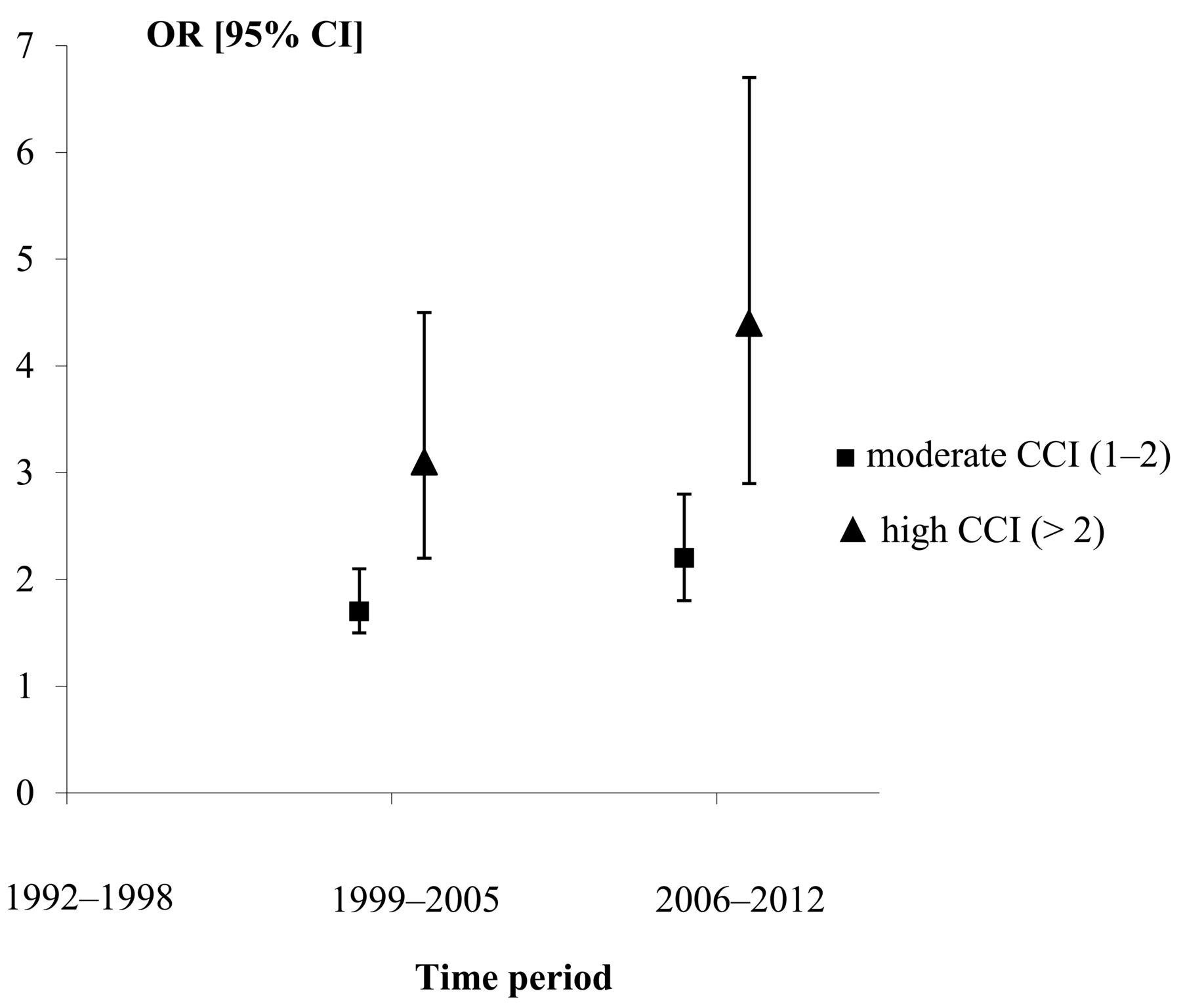
Temporal trends in Charlson Comorbidity Index (CCI) associated with total hip arthroplasty in patients with inflammatory arthritis. Three time periods, investigated using logistic-regression analysis, where a low score is the comparison group and 1992–1998 the baseline time period (adjusted for age, sex, diagnosis, level of education, and income).
Early postoperative mortality
In total, 3088 deaths (46%) occurred in the study cohort during the entire followup period. Twenty-five patients (0.4%) died within 0–90 days, giving a 90-day unadjusted survival rate of 99.6% (CI 99.5–99.8). An additional 28 patients died within 91–180 days after surgery, resulting in an unadjusted 180-day survival rate of 99.2% (CI 98.9–99.4). Unadjusted survival after 10 years was 65.4% (CI 64.2–66.7) in the entire cohort.
Early unadjusted survival differed significantly between the group with a CCI level > 2 (high) and the group with level 0 (low). Unadjusted 180-day survival was 99.6% (CI 99.3–99.9) in the group with low comorbidity, whereas it was 99.2% (CI 98.9–99.4) in the group with moderate comorbidity, and 97.0% (CI 94.8–99.2) for patients with a high degree of comorbidities (Figure 2).
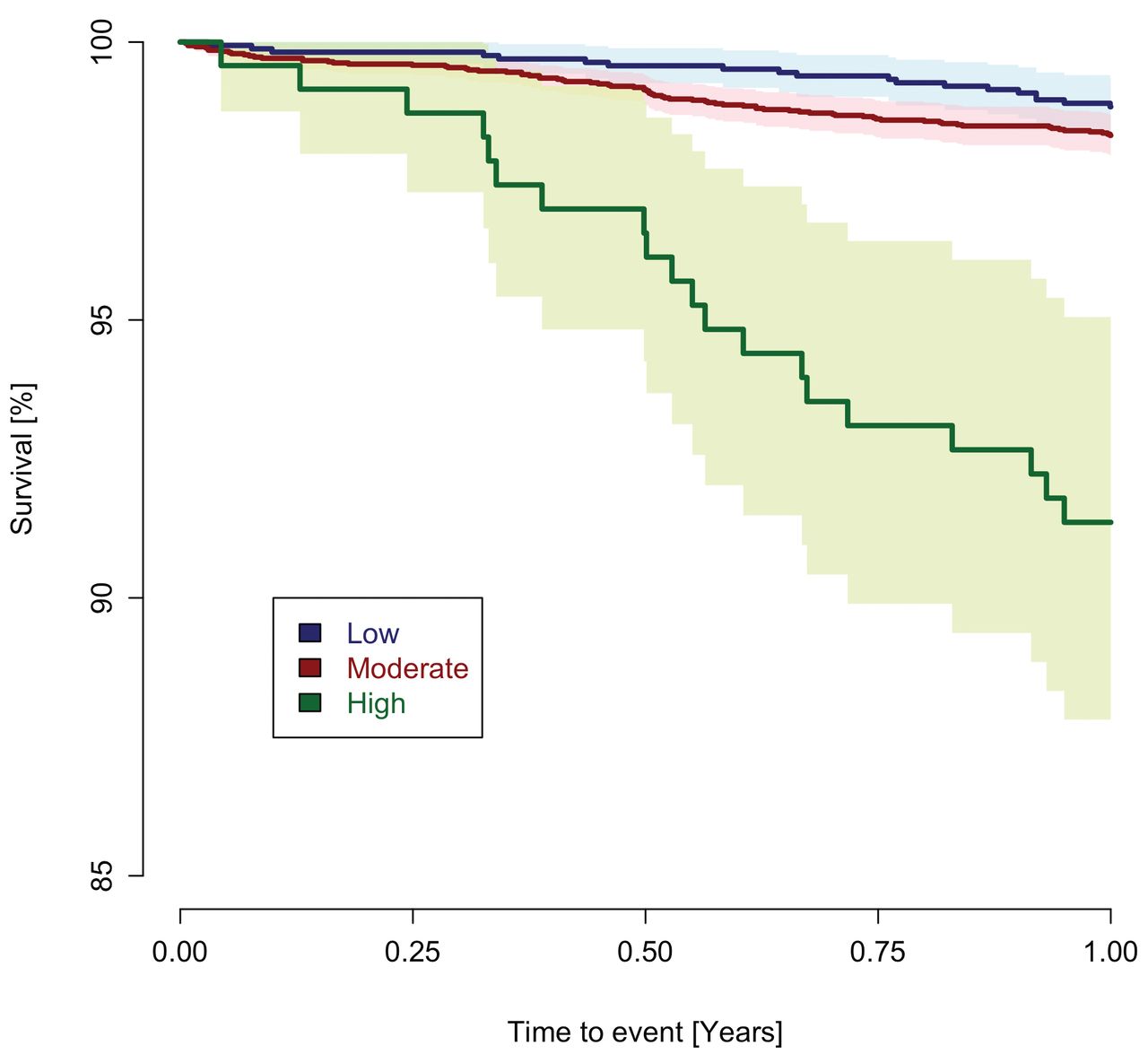
Mortality up to 1 year after total hip arthroplasty in patients with inflammatory arthritis, stratified into 3 different categories of medical comorbidity (Charlson Comorbidity Index: low, moderate, and high). Unadjusted survival according to Kaplan-Meier.
The HR for the risk of death in various time periods after the index procedure was calculated after adjustment for age, sex, type of inflammatory condition, comorbidity, time period, and socioeconomic status. We found that advanced age was associated with an increased risk of death within 90 days after surgery [> 75 yrs compared with < 60 yrs (adjusted HR 10.7)]. A high CCI (adjusted HR 9.0) increased the risk of death compared with patients with a low score (Table 2).
HR for mortality 0 to 90 days after THA. Twenty-five patients died within that period.
The covariates associated with an increased risk of death within the second time period, i.e., 91–180 days, were mostly the same as those described for the time period 0–90 days. An age between 60–75 years (adjusted HR 4.6) and above 75 years (adjusted HR 11.5) were both associated with an increased risk of death 91–180 days after THA compared with an age < 60 years (Table 3). A high degree of medical comorbidity according to the CCI also increased the risk of death within this second time period (adjusted HR 6.7) when compared with a low CCI score (Table 3).
HR for mortality 91 to 180 days after THA. There were 28 deaths in that period.
Early mortality in different time periods
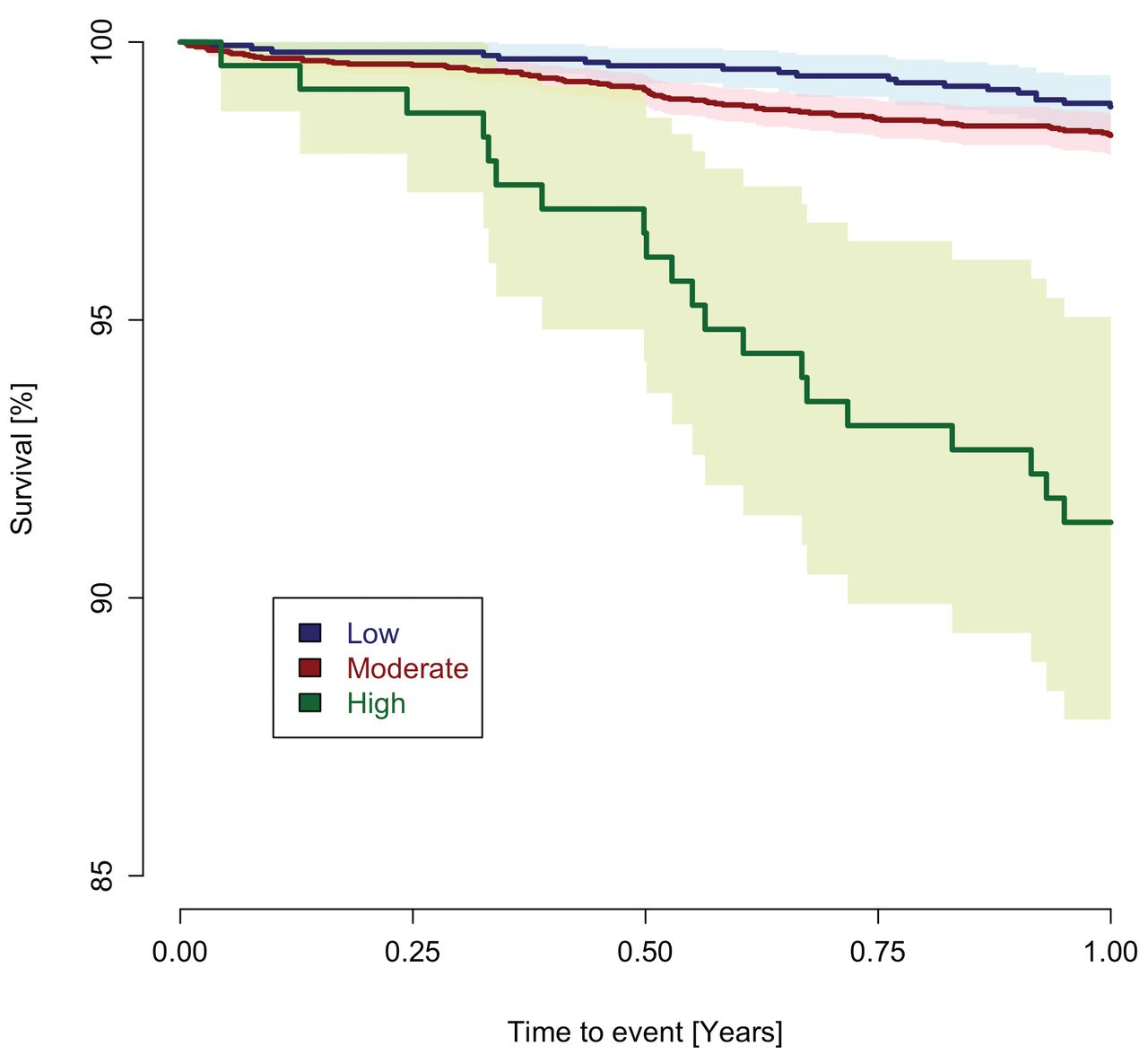
Unadjusted 180-day survival was 98.9% (CI 98.6–99.3) during the first observation period, ranging from 1992 to 1998. From 1999 to 2005, unadjusted 180-day survival increased to 99.5% (CI 99.2–99.8), and it was 99.5% (CI 99.0–99.9) from 2006 to 2012. Multivariable analyses of the risk of mortality up to 90 days from the index date indicated no statistically significant differences between the 3 time periods. Between 91 and 180 days, the multivariable analyses showed a trend toward a lower risk of death during the period 1999 to 2005 compared with the preceding period (HR 0.4), but this finding was of borderline statistical significance (p = 0.07; Table 3 and Figure 3).

Mortality up to 1 year after total hip arthroplasty in patients with inflammatory arthritis, stratified into 3 different time periods: 1992–1998, 1999–2005, and 2006–2012. Unadjusted survival according to Kaplan-Meier.
Risk factors for readmission for CV reasons within 90 days
A large proportion of patients was readmitted to the hospital within 90 days after the index procedure (n = 2021, 30.2%). We identified 52 (0.8% of the study population) readmissions for CV reasons within 90 days. Advanced age was a risk factor for the adjusted HR for readmission for CV reasons within 90 days after the index procedure [60–75 yrs (adjusted HR 4.2) and > 75 yrs (adjusted HR 10.6) compared with < 60 yrs]. A high CCI [adjusted HR 3.4] was associated with an increased risk of readmission for CV reasons when compared with a low CCI (Supplementary Table 3, available online at jrheum.org).
DISCUSSION
Early mortality after THA in patients with IA
Our study indicates that the presence of medical comorbidity according to the CCI and an age above 75 years were associated with an increased early adjusted risk of death in patients with IA after THA. We also found that patients with IA who received THA in the most recent observation period from 2006 to 2012 had more severe medical comorbidities when compared with the first period, 1992 to 1998. Despite this, the early mortality was not increased during later periods.
We focused on mortality during the first 6 postoperative months because deaths within this timeframe are more likely related to the surgical procedure than deaths occurring thereafter. The relatively high mortality in our study population during the remaining followup period is noteworthy, and this high mortality in our cohort is probably due to the inflammatory condition per se, rather than a consequence of the THA11,20.
We found a mortality of 0.4% during the first 90 days after the index procedure, and a 180-day mortality of 0.8%. This number is slightly lower than most 90-day mortalities reported in the literature on early postoperative mortality in patients with IA receiving a THA. Ravi, et al reported a 90-day mortality rate of 0.8% in 1163 patients with RA after THA4. Parvizi, et al analyzed 1072 patients with RA after THA and found a 30-day mortality of 0.75%10. Stundner, et al described a 30-day mortality of 0.2% in 5400 patients with RA6. A comparison of elective THA surgery in patients with systemic lupus erythematosus (SLE) or RA indicated that those with SLE had a higher in-hospital mortality (0.3%) than those with RA (0.1%)7.
The early mortality in our cohort of patients with IA was higher than the early mortality found in patients undergoing a THA as a result of OA15,21. However, other authors comparing early postoperative mortality after THA in patients with IA or OA find no strong evidence for increased mortality in the IA population. In a systematic review, Singh, et al concluded that RA was not associated with an increased 30-day and 90-day mortality after THA22. Concerning 30-day mortality, some contemporary studies do not find any difference in early postoperative mortality when comparing patients with RA to patients with OA5,6,7.
The effect of comorbidity on early mortality
Importantly, our study setting enabled us to identify and to adjust for medical comorbidities, and the high degree of medical comorbidities in this population is remarkable. In a systematic review, Berstock, et al identified 32 studies published on the topic of mortality after THA surgery over the last 10 years23. These authors reported a 90-day mortality of 0.65% in patients with OA after THA and also found a temporal trend toward reduced mortality rates despite an increasing degree of comorbidity23. We also observed a decrease in mortality in the latest observation period of 2006–2012 despite increasingly comorbid patients, but — as in the above-cited study — this observation was not statistically significant. However, the finding of slightly lower or at least constant early mortality is reassuring for patients with IA undergoing elective THA. The reasons for this observation are certainly multifactorial, and changes in surgical technique and improved perioperative care and anesthesia management may have contributed.
The observed increase in the comorbidity burden over time in patients with IA undergoing THA surgery is paralleled by an increased comorbidity in patients undergoing THA for other reasons. Several other studies report an increase in the comorbidity burden over time in unselected patients undergoing THA24,25,26,27,28. We found that a perioperative high CCI compared with a low score increased the risk of early mortality after THA. The CCI has been shown to correlate with the risk of morbidity and mortality in surgical patients13. However, this classification system has not been validated in patients with IA undergoing THA. Singh, et al analyzed 90-day complications after THA in patients with unselected operative diagnoses26. He reported that a higher American Society of Anesthesiologists (ASA) score (III–IV) was a risk factor for cardiac events. Mahomed, et al studied 61,568 patients after elective primary THA for reasons other than a hip fracture29. Patients with a CCI of 1 or more had a greater risk of adverse outcomes, particularly 90-day mortality. Kirksey, et al documented the association of a high Deyo comorbidity index with an increased in-hospital mortality in a large sample of unselected patients after THA in a US cohort28.
Other risk factors associated with early mortality
Unsurprisingly, we identified advanced age as a risk factor for early mortality. Apart from the obvious fact that death is more probable the older the patient, this observation may stem from the higher degree of preexisting medical comorbidities in elderly patients, and the lesser ability of elderly patients to cope with the hemodynamic strains associated with major surgery. Advanced age as a risk factor for adverse outcomes after elective THA is described by other authors29.
In our investigation, socioeconomic factors were not statistically significantly associated with the risk of early mortality, although other studies indicated that socioeconomic background exerts a profound influence on mortality over longer followup periods in Swedish cohorts30. A study of a Swedish population of patients with RA concluded that “socioeconomic class had no effect on treatment or outcome […]”31. However, because socioeconomic background is known to have a profound influence on short-term and longterm mortality, it may be that the moderate size of our study population in combination with the relatively low early mortality leads to insufficient statistical power to detect effects of variations in socioeconomic background variables.
It has been suggested that cemented fixation of THA increases perioperative mortality when compared with uncemented THA32. This suggestion has been strongly opposed for several reasons, and among other shortcomings, the lack of adjustment for medical comorbidities and socioeconomic background variables have been pointed out as weaknesses of that study33. It would have been interesting to investigate this issue in the context of a cohort of patients with IA, but the number of events per fixation subgroup was not high enough to enable such analyses (data not shown).
Re-admissions to hospital
A very high proportion of our cohort (30%) was re-admitted to hospital within 90 days after the index date. Because CV morbidity and mortality are high in patients with IA, we investigated the endpoint early re-admissions to hospital for CV reasons. We found that only a minority of patients with IA were re-admitted for such reasons, and risk factors for re-admissions for CV reasons were an age of 60 years and above and a high CCI. These findings are supported by data on the re-admission after THA or total knee arthroplasty in patients older than 65 years, where age and CV disease were associated with the risk of early re-admission34. The finding of comorbidity as a predictor of 30-day re-admission after THA was also described to be dependent on ASA grade35.
Strengths and limitations
Shortcomings of our study were related to its observational, registry-based design, with the typical inherent limitations concerning registration completeness, selection bias, and thus compromised validity. The proportion of higher comorbidity scores increased during the entire study period. It is reasonable to assume that this phenomenon is in part due to the introduction of reimbursements based on diagnosis-related groups24. Thus, observations of increased comorbidity burdens over time must be interpreted with caution.
There are confounders we were unable to adjust for, such as smoking habits, body mass index, and medication, which all exert an influence on our primary outcome. On the other hand, strengths of our study included the nationwide population-based design, a relatively large sample size, and adjustment for the important confounders medical comorbidity as well as socioeconomic background. Owing to the design of the Swedish registries, we had a high degree of registration completeness, and apart from persons who emigrated, near completeness of followup. The Swedish IPR was launched in 1964 but complete coverage did not begin until 1987. Currently, more than 99% of all somatic and psychiatric hospital discharge diagnoses are registered in the IPR16. Our followup period of almost 10 years was rather long and the investigated time span from 1992 to 2012 allowed for direct comparisons between different calendar periods.
We found that medical comorbidity and age above 75 years were important risk factors for early mortality after THA in patients with IA. This information is important when discussing the risks for such patients scheduled for THA, and especially in those with medical comorbidities. Awareness of such risk factors associated with increased early mortality may alert orthopedic surgeons to patients who are potentially at risk, and this awareness could thus contribute to improved perioperative care.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.
Acknowledgment
We thank all the Swedish orthopedic surgeons and secretaries who contributed data.
- Accepted for publication March 8, 2016.








{kind=link}
{kind=link}
{kind=link}