

Abstract
Objective. Chronic inflammatory rheumatic diseases are associated with accelerated atherosclerosis, but data in ankylosing spondylitis (AS) are limited and the relative contribution of inflammation versus classical cardiovascular (CV) risk factors remains a matter of controversy. We addressed this in an original study and a metaanalysis of previous studies.
Methods. Atheromatic plaques in carotid and femoral arteries, carotid hypertrophy [intima-media thickness (IMT), cross-sectional area], and carotid stiffness by ultrasound, as well as aortic stiffness by pulse wave velocity, were examined in consecutive nondiabetic, CV disease (CVD)-free patients with AS. Healthy individuals carefully matched 1:1 with patients for age, sex, smoking habits, hyperlipidemia, and hypertension served as controls. A metaanalysis of original studies that examined subclinical atherosclerosis in patients with AS versus controls with comparable CVD risk factors was also performed.
Results. Carotid and femoral atheromatic plaques were slightly less prevalent compared with controls in a contemporary cohort consisting of 67 patients with AS (82% men), aged 47.5 ± 12.5 years (mean ± SD), with a median disease duration of 12 years and a Bath AS Disease Activity Index (BASDAI) of 1.8 (interquartile range 0.4–3.6), of whom 66% were receiving anti-tumor necrosis factor (TNF) treatment. Carotid hypertrophy and stiffness, as well as aortic stiffness, were similar between patients and their matched controls. Metaanalysis of all published studies revealed a significantly increased carotid IMT, but not plaque burden, in AS versus controls. Notably, however, increased IMT was not evident in studies involving patients with low disease activity (mean BASDAI < 4) or in those studies that included > 50% of patients treated with anti-TNF.
Conclusion. Low AS disease activity is not associated with accelerated atherosclerosis.
The role of chronic systemic inflammation in the pathogenesis of accelerated atherosclerosis in patients with rheumatic diseases has been well described. Underlying mechanisms that promote the atherosclerotic process include increased prevalence of classical cardiovascular (CV) disease (CVD) risk factors and metabolic syndrome, alteration of lipoprotein concentrations, oxidative stress, as well as increased inflammatory cell-mediated direct endothelial injury and dysfunction1. According to the European League Against Rheumatism (EULAR) recommendations2, patients with rheumatoid arthritis (RA) have a 1.5-fold increased risk of CVD than the general population and require more aggressive CV screening and management. Even though data on ankylosing spondylitis (AS) are more limited, these patients also have increased CVD morbidity and mortality compared with the general population3,4,5, a finding that cannot be fully attributed to the higher prevalence of classical CVD risk factors and metabolic syndrome6,7,8,9,10.
Several studies have focused on the effect of AS disease per se on endothelial dysfunction and the progress of atherosclerosis7,10⇓⇓⇓⇓⇓⇓⇓⇓⇓ – 20,21,22,23,24,25,26,27,28,29. A metaanalysis performed in such studies published up to 2009 concluded that atherosclerosis was accelerated in patients with AS, as evidenced by significantly greater intima-media thickness (IMT) values compared with controls9. However, this metaanalysis9 included only 4 case-control studies examining carotid IMT, and interestingly, results from 3 of them suggested differently7,12,15. Along this line, 6 subsequently published original case-control studies showed that IMT in AS was not increased20,22,24,26,27,28. Discrepancies are perhaps because of the synergetic damaging effect of chronic inflammation and the different concomitant CVD risk factors across studies. On the other hand, an important limitation of all published studies so far is that none used a strict 1:1 matching methodology between patients with AS and healthy subjects for every classical CVD risk factor.
Therefore, to safely test the hypothesis that subclinical atherosclerosis (atheromatic plaques, arterial hypertrophy, and stiffness) develops earlier in patients with AS compared with healthy individuals, we conducted a case-control study strictly 1:1 matched for classical CVD risk factors. In a further effort to dissociate the involvement of disease status per se from that of classical risk factors, we also performed a metaanalysis of those original studies that examined subclinical atherosclerosis in patients with AS versus controls with comparable CVD risk factors.
MATERIALS AND METHODS
Study population and study design
Consecutive consenting patients attending the Laikon Hospital’s rheumatology outpatient clinics between 2011 and 2013, who had been diagnosed with AS according to the New York criteria30, were candidates for our study. Exclusion criteria included clinical CVD, diabetes mellitus (already diagnosed by a physician or 2 fasting plasma glucose levels on different days > 125 mg/dl or HbA1c > 6.5%), malignancy, chronic renal failure, or other concomitant severe disease [i.e., human immunodeficiency virus (HIV) infection]. Indices of AS disease activity and function, namely the Bath AS Disease Activity Index (BASDAI)31 and the Bath AS Functional Index (BASFI)32, as well as the Health Assessment Questionnaire Disability Index (HAQ-DI)33, were calculated. Erythrocyte sedimentation rate, serum C-reactive protein, glucose, total cholesterol, low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), and triglycerides measured within 3 months from examination were also recorded.
Eighty-one patients, aged 46.8 ± 13.3 years, 85.2% men, were enrolled; 67 of them could be matched 1:1 with healthy controls for age (± 2 years), sex, smoking habits, hyperlipidemia (defined as diagnosis by a physician or LDL fasting plasma levels > 160 mg/dl), and hypertension (HTN; defined as diagnosis by a physician or blood pressure levels > 130/80 using a 24-h monitoring device). The remaining 14 patients meeting inclusion criteria could not be effectively 1:1 matched to healthy controls. Sixteen other patients had been excluded because of coronary heart disease and/or cerebrovascular insult (n = 5), diabetes mellitus (n = 8), concomitant HIV infection (n = 1), severe heart failure (ejection fraction = 20%, n = 1), and chronic lymphocytic leukemia (n = 1). Our study was approved by our Institutional Scientific Board, and informed consent was obtained from patients and controls according to the Helsinki Declaration.
Assessment of subclinical atherosclerosis
Patients and controls abstained from food, drink, or any medication for 12 hours prior to the comprehensive study of (1) subclinical atheromatosis, (2) carotid hypertrophy, and (3) common carotid artery (CCA) elasticity and aortic stiffness. Subclinical atheromatosis was assessed by the presence of atheromatic plaques in a total of 8 arterial beds (left and right, common and internal, carotid arteries and carotid bulb; and both common femoral arteries) by ultrasound (US). Atheromatic plaques were defined as the local increase of the IMT of > 50% compared with the surrounding vessel wall, an IMT > 1.5 mm, or local thickening > 0.5 mm34. Carotid hypertrophy was estimated by IMT (adjacent to plaques when present) and cross-sectional area (CSA) in both the right and left common carotid arteries by US35. The common carotid arteries were scanned in both transverse and longitudinal planes, and IMT measurements were performed using automatic IMT measurement software. Carotid elasticity was assessed by US and aortic stiffness by carotid-to-femoral pulse wave velocity (PWV) and pressure wave reflections by augmentation index using the Sphygmocor device (AtCor Medical) and pulse wave analysis methodology36. Carotid elasticity was assessed by echocardiogram-gated US B-mode derived images that were used for the measurement of both left and right common carotid internal diameters during systole (CDs) and diastole (CDd). Strain was calculated according to the following formula:
 Young’s modulus was calculated as:
Young’s modulus was calculated as:

Measurements were performed by a single experienced technician (GK) using high-resolution B-mode US (Vivid 7 Pro, GE Healthcare) with a 12 MHz linear matrix array transducer. All measurements were performed twice and the mean was recorded; all measurements exhibited high test-retest correlation coefficient (> 0.80), suggesting very good intraobserver reproducibility. The coefficients of variation for all the herein reported vascular biomarkers ranged from 0.02 to 0.08.
Statistics
Normality of sample distribution was examined by the Kolmogorov-Smirnov test. Continuous, normally distributed variables are expressed as means and SD, and analyzed using the paired Student t test. Continuous, not normally distributed variables are expressed as median and 25th and 75th percentile values, and analyzed using the Mann-Whitney U test. Categorical variables are shown in percentiles and were analyzed using the chi-square test. SPSS version 21 was used for all analyses and significance was defined as p < 0.05 in all cases.
Literature search and study selection for metaanalysis
Two researchers (AK and KM) independently performed a thorough search of Medline/PubMed, Cochrane, and Scopus databases for original cross-sectional controlled studies evaluating subclinical CVD in patients with AS published in English from January 2000 through July 2014. Search terms included: “ankylosing spondylitis,” “cardiovascular disease,” “atheromatosis,” “atherosclerosis,” “IMT,” “arterial stiffness,” and “PWV.” Any disagreements between the reviewers were resolved by consensus. For studies that published more than 1 article based upon overlapping groups of participants with the same outcome measure and study design, we included only the study with the largest number of participants. Case-control studies were excluded. These were also excluded: studies including patients with clinical CVD, giving inadequate information on study population, providing inadequate data for statistical analysis [no SD or using median and interquartile range (IQR)], or studies in which patients with AS and controls differed significantly in either age, sex, or any classical CVD risk factor (a flow chart of the selection of included articles is available from the authors on request). Information on the following items was extracted from each study with the use of a standardized form: design, sample size, population characteristics (age, sex, prevalence of CVD risk factors, blood pressure levels, lipid profile), and indices of subclinical atherosclerosis examined (carotid plaques, carotid IMT measurements, indices of carotid and aortic stiffness). For patients with AS, disease duration, BASDAI and BASFI scores, and the use of biological therapy were also recorded. Studies meeting the above criteria were stratified according to the mean level of disease activity (BASDAI < or ≥ 4), and the proportion of patients receiving anti–tumor necrosis factor (anti-TNF) biological therapy (≤ or > 50%).
The metaanalysis was conducted in R software using the “metafor” package as downloaded from Comprehensive R Archive Network repository (cran.r-project.org)38. Data were analyzed using random-effects models because of heterogeneity between studies, which was assessed by I2 and Cochran Q tests. The Egger test was considered to assess the presence of asymmetry in the funnel plots. The outcome variables for the metaanalysis were the overall IMT (average IMT of right and left CCA), right IMT, and carotid plaques. In studies in which the overall IMT was not reported, the average over right and left IMT was considered.
RESULTS
Original study
As shown in Table 1, the mean ± SD ages of the 67 patients and 67 control subjects were 47.54 ± 12.47 years and 47.78 ± 12.69 years, respectively, whereas the median disease duration was 12 years. Thirty-three percent of participants in each group had HTN, 15% had hyperlipidemia, and 55% were smokers. Mean blood pressure levels and body mass index were also similar between the 2 groups. Patients with AS were of low current disease activity and good functional class (BASDAI 1.8, IQR 0.4–3.6; BASFI 2, IQR 0.9–2.8; HAQ-DI 0.13, IQR 0–0.5), and the majority (66%) was receiving anti-TNF treatment.
Demographics and clinical characteristics of patients with AS and healthy controls matched 1:1 for age, sex, and classical CVD risk factors. Data are mean ± SD or median (interquartile range) unless otherwise specified.
As shown in Table 2, all studied variables were comparable between patients with AS and controls. Carotid and/or femoral plaques were slightly increased in healthy subjects, albeit not reaching significance (plaques present in 23 patients and 32 controls, p = 0.114; Table 2). IMT, the main variable of arterial hypertrophy, was 0.79 ± 0.22 and 0.80 ± 0.20 in the left CCA versus 0.73 ± 0.16 and 0.75 ± 0.21 in the right CCA for patients and controls, respectively (p = 0.784 for left CCA and 0.421 for right CCA). PWV was 7.64 ± 1.7 m/s in patients versus 8.03 ± 1.92 m/s in controls (p = 0.232), and Augmentation Index was 18.58 ± 13.31% versus 17.52 ± 14.16% (p = 0.656; Table 2). By univariate regression analysis, none of the disease variables, such as duration and activity or anti-TNF treatment, were associated with any of the vascular indices.
Vascular indices of patients with AS and healthy controls matched 1:1 for age, sex, and classical CVD risk factors. Data are mean ± SD or n unless otherwise specified.
Metaanalysis
We retrieved 23 studies evaluating subclinical CVD in AS; 14 of them11,12,15,18,20⇓⇓⇓⇓⇓⇓⇓⇓ – 29 fulfilled our inclusion criteria. One study was excluded because of possible duplicated reports20. Another study was subsequently excluded because it only examined aortic stiffness (PWV), but not carotid hypertrophy or atheromatosis11. Variation of stiffness indices examined throughout the studies did not allow metaregression analysis, because data on each index were too limited. Therefore, 12 studies were included that involved a total of 521 patients and 445 matched controls, providing adequate information on IMT from both or either right CCA and/or presence of plaques for both patients and controls. Patient characteristics and results from each of the included studies are provided in Table 3.
Characteristics and results of 12 published studies included in the metaanalysis.
Regarding carotid hypertrophy, we found that patients with AS had significantly increased overall IMT (i.e., average of left and right CCA) compared with matched controls (mean 0.046, 95% CI 0.015–0.077; Figure 1), as well as increased IMT of only the right CCA (0.034, 95% CI 0.004–0.064). On the other hand, analysis of those 5 studies examining the presence of carotid plaques in AS revealed no statistical difference in the relative risk (RR) for the presence of plaques between the 2 study groups (RRpooled = 1.07, 95% CI 0.48–2.37), meaning that the chance of observing plaques in patients with AS is 1.07 times greater as compared with controls (Figure 2). We then performed a sub-metaanalysis of those studies involving patients with well-controlled AS with a mean BASDAI score < 4 and found that the IMT was not increased compared with controls (0.016, 95% CI −0.05 to 0.037, p = 0.1343). In contrast, metaanalysis of studies with patients with AS of moderate or high disease activity (BASDAI score ≥ 4) continued to show significant difference in IMT between cases and controls (0.097, 95% CI 0.077–0.117, p < 0.001; Table 4). Similar findings were derived from a subgroup metaanalysis of those studies in which > 50% of patients were receiving anti-TNF therapy; the difference in IMT between patients and controls did not reach significance (0.018, 95% CI −0.042 to 0.078, p = 0.5766; Table 4). In contrast, in the group of studies with 0–50% proportion of patients receiving anti-TNF treatment, IMT measurements were significantly increased in AS compared with controls (0.064, 95% CI 0.019–0.108, p = 0.0054).
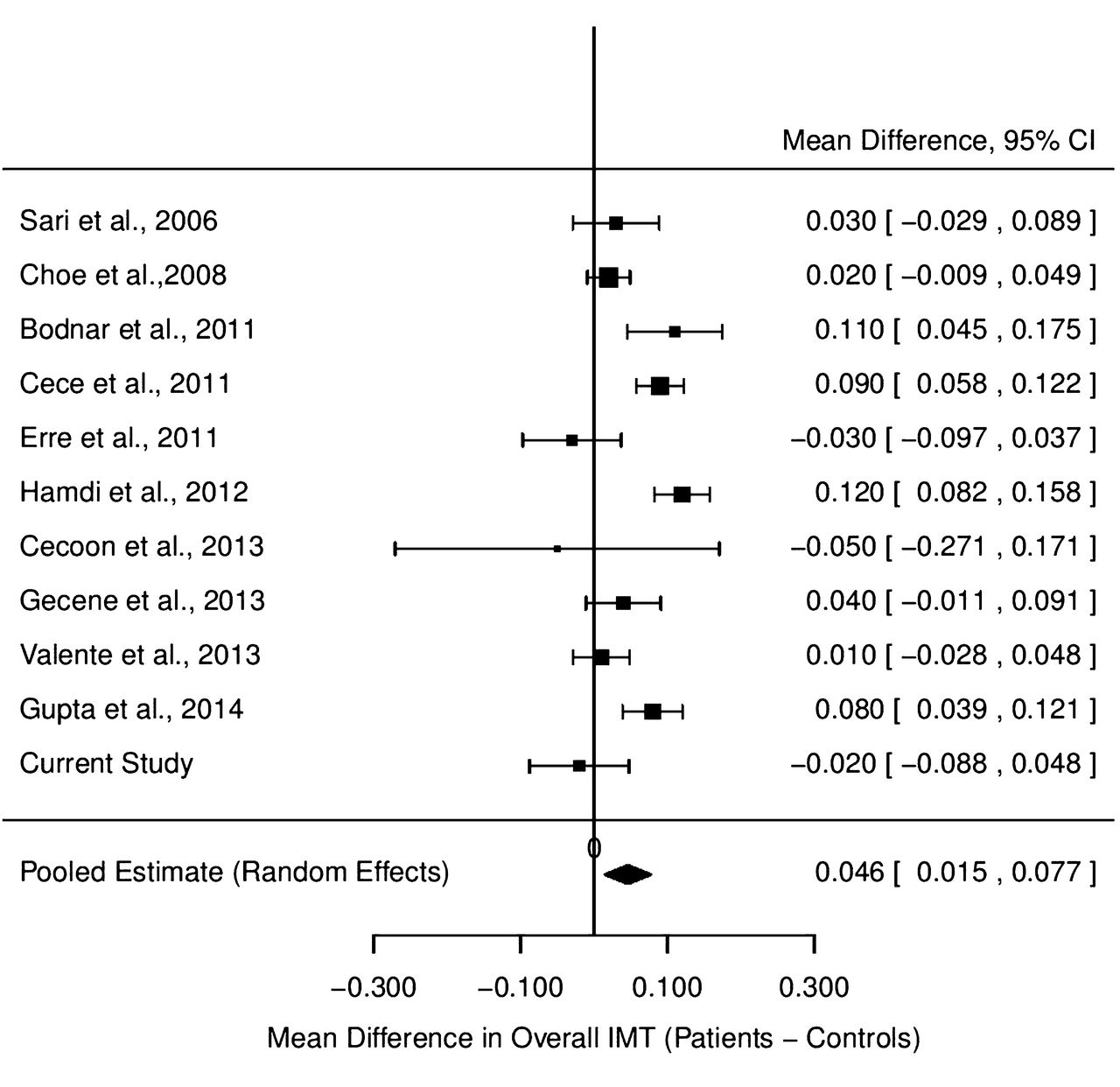
Pooled difference in overall mean IMT (right and left CCA) between patients and controls. IMT: intima-media thickness; CCA: common carotid artery.
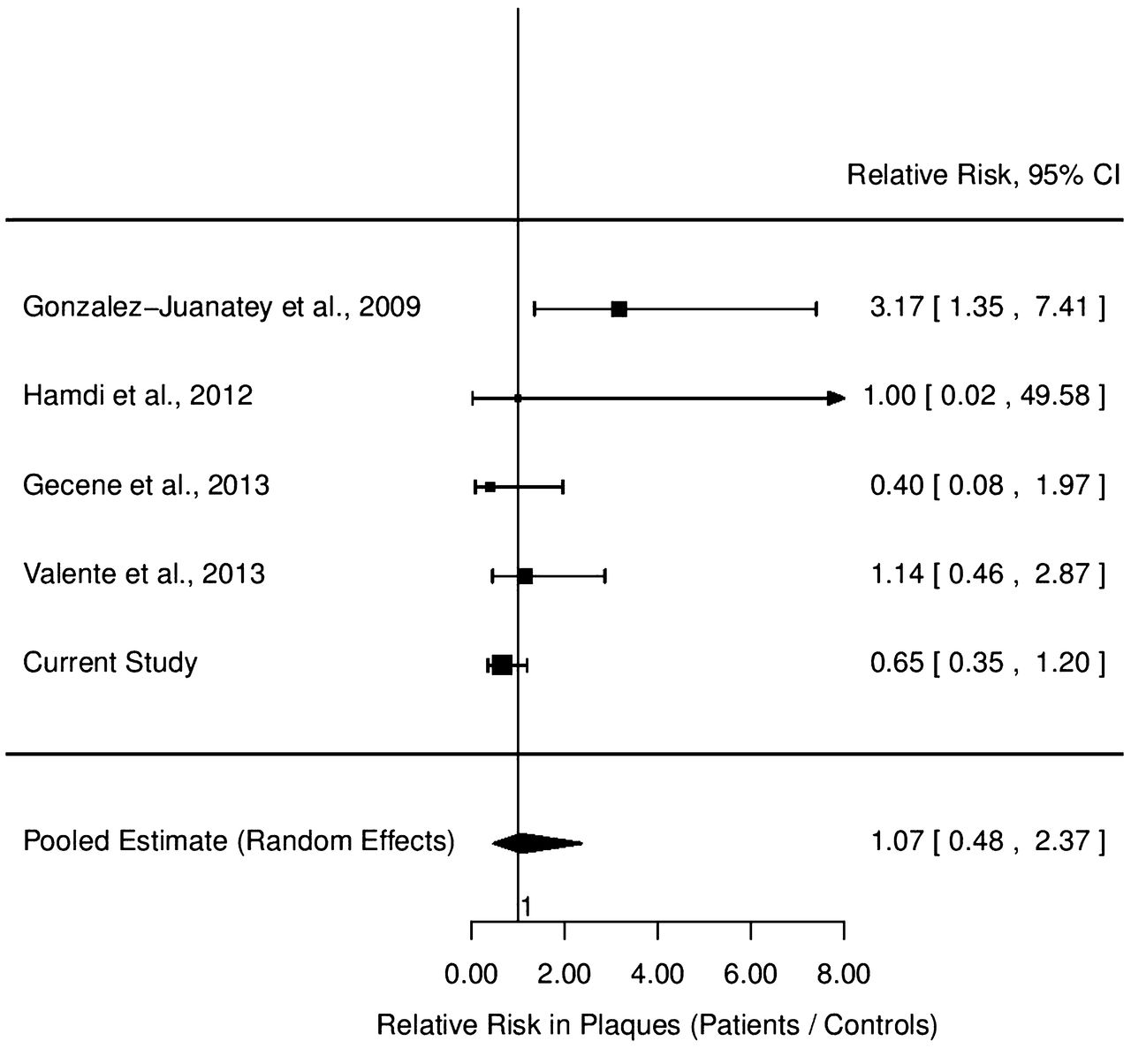
Pooled difference of the relative risk for the presence of carotid atherosclerotic plaques between patients with ankylosing spondylitis and controls.
Pooled difference in overall IMT (mean of right and left CCA) in subgroups of studies stratified by the level of disease activity as measured by BASDAI or the proportion of patients treated with anti-TNF. Values are mean (95% CI) unless otherwise specified.
DISCUSSION
Our original data clearly show that in patients with AS with low disease activity, subclinical atherosclerosis — in terms of atheromatosis, carotid hypertrophy, and arterial stiffness — is not accelerated compared with apparently healthy individuals. To avoid an underestimation of the effect of chronic inflammation, and because atherosclerosis is a chronic long-lasting process, we elected to use the New York criteria for AS diagnosis instead of the Assessment of Spondyloarthritis international Society axial criteria39, which include more early patients. Our results cannot be directly compared with those of previous studies, because none of them consisted of a strict 1:1 matching for each of the classical CVD risk factors. Notably, our metaanalysis confirmed our original data because the subgroup analysis of studies involving patients with a BASDAI < 4 showed that carotid IMT is similar to controls. As expected, however, overall and subgroup metaanalysis revealed that active AS disease is indeed associated with increased carotid IMT.
Chronic systemic inflammation promotes all phases of atherosclerosis and can explain the harmful effect of active AS disease on arterial remodeling. Interestingly, the lack of increased plaque burden in the metaanalysis may be explained by the relatively young age of the patients examined who had AS (mean of 37.7 ± 10.8 yrs); an interaction between age and chronic inflammation has been described40. Alternatively, it may be a result of the relatively small number of available studies and cumulative sample size. Plaque formation represents a more advanced stage of atheromatosis than IMT increase, and it is a cumulative result of the effect of many pro-atherogenic factors. Only 1 study involved patients with high disease activity with a mean age of more than 50 years, and in this study, carotid plaques were significantly more prevalent than controls18. On the other hand, the presence of increased IMT does not per se suggest increased atheromatosis, but it may also be attributed to subclinical vasculitis and/or wall hypertrophy. Such a mechanism of arterial dysfunction has been described in patients with RA, in whom active disease is associated with increased aortic inflammation compared with healthy subjects41.
The absence of increased carotid IMT in patients with AS with low disease activity could also be attributed to the resolution of vessel wall inflammation. It should be noted that the proportion of our patients receiving anti-TNF therapy is higher than what is commonly seen in clinical practice, but this is because of the fact that patients with severe AS are referred to our Tertiary Academic Hospital. Anti-TNF therapy appears to be involved in ameliorating vascular properties. Anti-TNF therapy in RA succeeded in reducing aortic inflammation along with disease activity, thus decreasing aortic stiffness measured by PWV41. Apart from the probable direct effect of TNF inhibitors on vascular inflammation, these agents affect lipid profile42 and antioxidative capacity of HDL43, and may even have a specific direct effect on the arterial wall. Nevertheless, reduction of systemic inflammation by anti-TNF agents seems to be the main reason for similar arterial features between patients with systemic inflammatory diseases and healthy individuals, and can explain the lack of increased carotid hypertrophy in patients with AS with low disease activity. A recent review by Tam, et al44 examining the effect of TNF antagonists on the progression of atherosclerosis and in reducing CV risk concluded that anti-TNF agents are probably effective in preventing or even reversing the progression of IMT in patients with systemic rheumatic diseases responding to treatment. Moreover, successful anti-TNF therapy seems to induce a persistent stable vascular function in the long term45.
Regarding carotid and/or aortic stiffness and vascular function in AS, variation of vascular indices examined did not allow metaanalysis of published data. In patients with AS in particular, published studies, while diverse, suggest that active AS disease causes impaired vascular elasticity and function14,16,17,19,46. However, our original data, as well as results from other studies, indicate that effective disease control, particularly by anti-TNF treatment, seems to reverse arterial stiffness and ameliorate functional arterial indices concurrent with reduction in clinical and laboratory inflammatory markers27,45,46,47,48. A recent study by Berg, et al examining the association between disease activity in AS and markers of vascular pathology concluded that patients with high AS disease activity present with a higher CVD risk49. Moreover, another recent 5-year followup study published by the same researchers and evaluating possible factors of CV risk supported that disease activity was related to elevated arterial stiffness and thus future risk of CV disease50.
To our knowledge, our metaanalysis is the first to examine carotid IMT in patients with AS and apparently healthy controls with comparable classical CVD risk factors. Moreover, this is the first metaanalysis to examine the presence of carotid plaques in AS. Limitations of our metaanalysis include the following: first, differences between patients and controls in some studies regarding age, sex, or CVD risk factors, although not significant, could have affected the final results. Second, concerning IMT calculation, information from published studies regarding methodology is lacking; only a few studies provided detailed information on the method used for IMT calculation and whether sites with plaques were included in IMT measurements. However, mean IMT values and SD from these studies lead us to conclude that this was the case. Finally, we were able to retrieve only 4 studies informing on the presence of plaques in AS, hence overall analysis regarding atheromatosis lacks statistical power.
The original results presented herein and the metaanalysis of previous findings show that subclinical atherosclerosis is not accelerated in patients with AS with low disease activity. However, inadequate control of disease activity results in increased carotid IMT and atheromatosis, especially in older patients. According to the EULAR guidelines for inflammatory arthropathies, the aggressive management of classical CVD risk factors in patients with AS is indicated2, but the present data clearly show that effective control of disease activity may minimize the CV burden of AS. This should be confirmed in prospective studies that are currently in progress.
Footnotes
Supported by Athens University Medical School grand ELKE 097.
- Accepted for publication July 15, 2015.








{kind=link}
{kind=link}