

Abstract
Objective. To analyze the role of interleukin 22 (IL-22) in rheumatoid arthritis (RA).
Methods. IL-22 serum levels were measured in 83 patients with established RA under treatment with disease-modifying antirheumatic drugs and in 30 healthy controls matched for age and sex. Patients were assessed for clinical and laboratory variables. Correlations of IL-22 serum levels with disease activity measures [Clinical Disease Activity Index (CDAI) and Disease Activity Score for 28 joints (DAS28)], serological markers, bone erosions, and demographic factors were assessed. Peripheral blood mononuclear cells (PBMC) from 30 patients with RA and 14 controls were purified and stimulated in vitro with phorbol myristate acetate (PMA)/ionomycin. IL-22 production by PBMC and in serum was investigated by ELISA.
Results. IL-22 levels were increased in patients with RA compared with controls (mean 432.37 pg/ml and 67.45 pg/ml, respectively; p < 0.001). Levels of IL-22 correlated with DAS28 and CDAI measures. Rheumatoid factor (RF) positivity was correlated with higher levels of IL-22 in patients with RA (mean 575.08 pg/ml; p = 0.001). The presence of bone erosions was associated with high IL-22 levels (p = 0.0001). PBMC stimulated with PMA/ionomycin expressed higher levels of IL-22 in patients with RA than controls but this was not significant (mean 584.75 pg/ml and 295.57 pg/ml; p = 0.553).
Conclusion. IL-22 is elevated in the serum of patients with established RA. Elevated serum IL-22 allows discrimination between patients with different clinical and laboratory measures and indicates the potential of IL-22 as an additional tool for assessment of activity in RA, particularly in patients with RF antibodies and longterm disease. IL-22 is associated with bone-destructive disease.
- INTERLEUKIN 22
- RHEUMATOID ARTHRITIS
- DISEASE ACTIVITY
- DISEASE ACTIVITY SCORE 28
- CLINICAL DISEASE ACTIVITY INDEX
Rheumatoid arthritis (RA) is a systemic chronic inflammatory autoimmune disease characterized by synovial proliferation and progressive damage of multiple joints. RA is a disease that mainly targets the synovial membrane, cartilage, and bone. At times, systemic manifestations may occur. It is associated with increased mortality and affects 0.4% to 1% of the population1. More than one mechanism could contribute to the disease. Cytokines are directly implicated in the pathogenesis of RA as part of a complex regulatory network related to specific immunological processes that promote autoimmunity, chronic inflammation, and tissue destruction2. T cell activation and migration are involved in these mechanisms, and these cells adopt a proinflammatory phenotype. RA has been thought to be a Th1- associated disorder3, but at present the Th17 phenotype has been identified and associated to RA4,5. Th17 cells have been clearly implicated in animal models of RA, i.e., collagen-induced arthritis (CIA)6, the SKG mouse7, and gene-targeted mice deficient in interleukin 1 (IL-1) receptor antagonist8. The functional role of these T cell subsets in human arthritis has been recently clarified5.
Th17 cell differentiation is regulated by the transcription factors signal transducer and activator of transcription 3 (STAT3), retinoic acid receptor-related orphan receptor-γt (RORγt), and aryl hydrocarbon receptor, and is driven by transforming growth factor-ß (TGF-ß), IL-1, and IL-6; IL-23 is required to expand and stabilize the cell population. In addition to IL-17A, Th17 cells produce IL-17F, IL-21, IL-22, and IL-26, as well as chemokines such as CC chemokine ligand 20 (CCL20; also known as MIP3α)9,10,11. Recently IL-17A production and IL-22 expression have been demonstrated to occur independently of TGF-ß signaling12.
IL-22 is a member of the IL-10 cytokine family and is related to different T cell subsets. IL-22 is presumed to play a role in pathogen defense, wound healing, and tissue reorganization, therefore IL-22 modulates tissue responses during inflammation. IL-22 is involved in the induction of an acute-phase response in vivo and chemokines and matrix metalloproteinases in vitro13. IL-22 takes part in the adaptive response by the activation of CD4 T cells and in the innate response by the activation of lymphocytes such as natural killer cells and lymphoid tissue inducer-like cells14. IL-22 signals through a heterodimeric receptor complex consisting of the IL-10R2 and IL-22R115,16. The IL-22R1 subunit is strongly expressed in the skin, kidney, and tissues of the digestive and respiratory systems and synovial fibroblasts13. Binding of IL-22 to this receptor leads to activation of STAT3 signaling cascades and Akt and mitogen-activated protein kinase pathways14. The role of IL-22 as a Th17-effector cytokine has been demonstrated and it is most highly expressed by this cell subset17. Expression of this proinflammatory cytokine is induced by intradermal injection of IL-22 in mice13. The functional role of IL-22 is also associated with chronic inflammatory diseases such as psoriasis, inflammatory bowel disease (IBD), and RA13,14,18,19,20. Both psoriasis and IBD predispose to spondyloarthritis, including axial disease, therefore examination of this cytokine was relevant in ankylosing spondylitis21. IL-22 has also been implicated in the pathogenesis of reactive arthritis22.
In IBD, IL-22 expression was detectable in CD4-positive T cells and was related to the expression of other inflammatory cytokines18. Increased levels of IL-22 in patients with psoriasis23, Sjögren’s syndrome24, and RA19,20,25 have been described, suggesting that it has proinflammatory properties and is important in these autoimmune diseases13. In RA, IL-22 possibly induces the proliferation of synovial fibroblasts and production of chemokines19. In animal models of collagen-induced arthritis, mice deficient in IL-22 were less susceptible to pannus formation and incidence of arthritis26. IL-22 levels have been associated to radiographic progression in RA20. Nevertheless, there are currently no studies demonstrating a positive correlation between levels of IL-22 and disease activity. We investigated serum levels of IL-22 in patients with RA to determine its relations to disease activity and severity.
MATERIALS AND METHODS
Study population
A total of 83 patients with RA (80 women, 3 men; mean age 53 ± 10.6 yrs) were recruited from the Department of Rheumatology at Hospital das Clínicas da Universidade Federal de Pernambuco (UFPE). Current medications were recorded (Table 1); 6 patients were taking biological agents (5 adalimumab and 1 etanercept). The diagnosis of RA was established by the presence of 4 or more American College of Rheumatology 1987 diagnostic criteria27. About 30 healthy volunteers matched for age and sex (mean age 44 ± 10.8 yrs) were included as controls, and all were free of any rheumatologic conditions. Peripheral blood samples were obtained from patients and controls.
Demographic, clinical, and laboratory presentation of the patients with rheumatoid arthritis.
Demographic, clinical, and laboratory data were collected from hospital records or by questionnaire and reviewed by experienced physicians. Table 1 presents demographic and clinical findings in patients with RA.
Laboratory features of patients with RA [erythrocyte sedimentation rate (ESR), rheumatoid factor (RF) positivity] were recorded. Individual disease activity was quantified using the Disease Activity Score for 28 joints (DAS28)28 and the Clinical Disease Activity Index (CDAI)29. Radiographs of hands were obtained from patients with RA and evaluated for the presence of erosions by an experienced rheumatologist blinded to the clinical data. All subjects gave written consent to participate. The study was approved by the ethics committee of the UFPE.
Peripheral blood mononuclear cells (PBMC)
PBMC were obtained from heparinized blood from healthy, nonsmoking donors who had not taken any drugs for at least 15 days before sampling, and were isolated by standard density-gradient centrifugation over Ficoll-Hypaque (GE Healthcare). Cells were counted in a Neubauer chamber, and cell viability was determined by the trypan blue exclusion method. Cells were used only when viability was > 98%.
PBMC cultures
PBMC (1 × 106 cells/well) from 30 patients with RA and 14 controls were cultured in 24-well plates in RPMI-1640 (Gibco) supplemented with 10% fetal bovine serum (Gibco), HEPES 10 mM (Gibco), and penicillin/streptomycin 200 U/ml (Gibco), and incubated at 37°C in a humidified 5% CO2 incubator. Cells were stimulated/not stimulated with phorbol myristate acetate (PMA) 100 ng/ml (Sigma) and ionomycin 1 μg/ml (Sigma). The supernatants were collected after 48 h and IL-22 levels were quantified.
Measurement of serum IL-22 levels
Cytokines in the supernatants of cultures and in sera were assayed with an ELISA kit according to the manufacturer’s recommendation (R&D Systems). The lower limit of detection for the ELISA IL-22 kit was 15 pg/ml.
Statistical analysis
Associations of serum IL-22 levels with clinical and laboratory measures of patients with RA were analyzed by univariate comparisons using nonparametric tests (Mann-Whitney tests). p < 0.01 was considered a significant association and p < 0.05 a suggestive association. Results are shown considering the mean value. All quantitative data were plotted with GraphPad Prism 3.02 software. Variables with p < 0.2 at univariate analysis were retained for multivariate logistic regression analysis.
Correlations between serum IL-22 levels and DAS28 and CDAI were evaluated using Pearson correlation analysis. This analysis was carried out with Origin 8.0724 software (OriginLab, Northampton, MA, USA).
RESULTS
Serum IL-22 levels in RA patients and controls
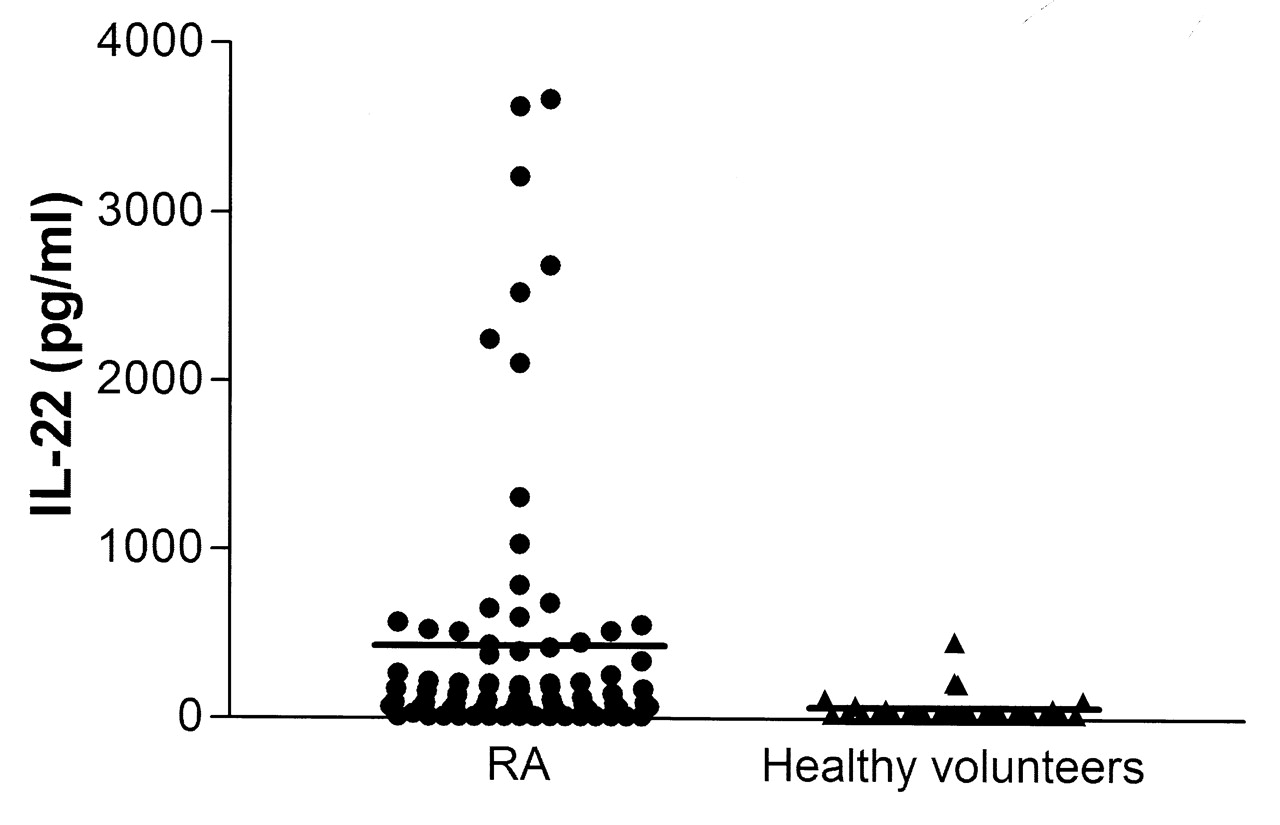
In total, 83 patients with RA and 30 healthy controls were included in our analysis. Serum IL-22 levels were significantly increased in RA patients compared with controls (mean 432.37 pg/ml and 67.45 pg/ml, respectively; p < 0.001; Figure 1). Serum levels of IL-17 were higher in patients with RA but this finding lacked statistical significance. No correlation was detected between IL-17 levels and disease activity (data not shown).

Serum interleukin 22 (IL-22) levels in patients with rheumatoid arthritis (RA) and controls.
Association of serum IL-22 levels and disease activity
Having found that IL-22 was elevated in patients with RA, we assessed whether serum levels of IL-22 correlated with disease activity.
There was significant correlation for serum IL-22 levels among the scores for DAS28 (r2 = 0.041, p = 0.037; Figure 2A) and CDAI (r2 = 0.062, p = 0.013; Figure 2B). Serum from patients with RA in clinical remission had significantly lower levels of IL-22 than serum from patients with mild, moderate, and severe disease.

Correlation between serum interleukin 22 (IL-22) levels from patients with rheumatoid arthritis and Disease Activity Score for 28 joints (A; r2 = 0.041, p = 0.037) and Clinical Disease Activity Index (B; r2 = 0.062, p = 0.013).
Correlations of serum IL-22 with RF positivity
Patients with RA who were positive for RF had significantly increased levels of IL-22 compared to seronegative patients (mean 575.08 pg/ml and 136.37 pg/ml; p = 0.001; Figure 3).

Correlation between rheumatoid factor (RF) positivity and levels of interleukin 22 (IL-22) in patients with rheumatoid arthritis.
Correlations of serum IL-22 levels with bone erosions
We assessed associations of IL-22 levels and presence of erosions. Serum IL-22 levels were higher in patients with bone erosions (mean 516.69 pg/ml) than in patients without erosions (mean 79.29 pg/ml; p = 0.0001; Figure 4).

Serum interleukin 22 (IL-22) levels in patients with rheumatoid arthritis and bone erosions.
The CDAI, DAS28, RF, and erosion variables were significantly associated with IL-22 by univariate analysis (p < 0.05). Therefore, these variables were subjected to multivariate logistic regression analysis. In the first analysis we considered DAS28, RF, and erosions; DAS28 and RF measures were independently associated with IL-22 levels (p = 0.046 and p = 0.013, respectively). Then we analyzed CDAI, RF, and erosions; CDAI and RF were also independently associated with IL-22 levels (p = 0.028 and p = 0.029, respectively).
IL-22 expression in PBMC following stimulation
Next we analyzed the IL-22 patterns in vitro following stimulation with PMA and ionomycin. We observed increased levels of IL-22 in patients with RA compared to controls.
PBMC from 30 patients with RA and 14 controls were stimulated in vitro with PMA and ionomycin. There was low spontaneous secretion of IL-22 in both groups (mean 17.66 pg/ml in patients with RA, 63.85 pg/ml in controls). The levels of IL-22 in supernatants of PBMC from patients with RA after stimulation were higher than in control PBMC (584.75 pg/ml and 295.57 pg/ml, respectively), but this finding was not statistically significant (p = 0.553; Figure 5).

Amounts of interleukin 22 (IL-22) from peripheral blood mononuclear cells of patients with rheumatoid arthritis (RA) and controls before and after stimulation with phorbol myristate acetate (PMA)/ionomycin.
DISCUSSION
In our study, IL-22 levels were increased in patients with RA compared with those of healthy controls. In this series the levels of IL-22 correlated with disease activity (by DAS28 and CDAI). Of note, when samples from patients with RA were separated into RF-negative and RF-positive groups, there were significant differences in IL-22 serum levels. There was significant correlation between higher levels of IL-22 and positive RF. IL-22 levels were higher in patients with bone erosions. PBMC stimulated with PMA/ionomycin expressed higher levels of IL-22 in patients with RA than in controls, but this finding was not significant.
It has been suggested that IL-22 might play a role in RA pathophysiology14,20,21,25,26,30,31. Elevated levels of IL-22 have been demonstrated in RA synovial tissues and the lining and sublining layers of rheumatoid synovium expressed higher levels of IL-22R119. Endogenous IL-22 plays a proinflammatory role in collagen-induced arthritis in C57BL/6 mice, and this cytokine appears to be important for osteoclastogenesis and regulates antibody production26. Our findings are in accord with these observations, and are also in agreement with a recent study that described increased plasma levels of IL-22 in 30 patients with established RA with a mean disease duration of 10.7 years, although the patients had not received immunomodulatory drugs for 2 months30. In contrast, all our patients were under therapy. In our study the mean disease duration was 10.5 years and most patients had active disease, as noted. Another recent study showed levels of IL-22 were increased in almost 50% of patients with very early and active RA, and revealed no difference for disease activity measures between the groups of RA patients with high IL-22 and those with normal IL-22 levels; the patients assessed had active disease. Both groups of patients had never been treated with disease-modifying antirheumatic drugs and glucocorticoids. Elevated levels of IL-22 at baseline were significantly associated with bone erosions20. We found higher IL-22 levels in patients with bone erosions of hands. This finding supports the potential role of IL-22 as a predictive marker of bone destruction in RA. However, previous data demonstrated that levels of IL-22 were elevated in patients with established disease as well as in patients with very early disease25. Our data show that patients with longterm disease have increased serum levels of IL-22, supporting the idea that this proinflammatory cytokine may take part in the chronic inflammatory process in established RA, but to a lesser degree in very early disease.
Although IL-22 has been described to have a mild proinflammatory effect in arthritis32 this is not in line with our observation that patients differ in their clinical inflammatory measurements (DAS28 and CDAI) according to serum levels of IL-22, showing a linear trend (Figure 2). Our study is the first to associate the levels of IL-22 with severity of disease according to DAS28 and CDAI, demonstrating statistical significance in patients with established disease. However, this is not in agreement with a previous study that found no correlation between plasma levels of IL-22 and DAS28 in a similar group of 30 patients in China30. Our study analyzed a higher number of patients (n = 83) and this inconsistency may arise in part from the influence of genetics in some ethnic groups on RA physiopathogenesis33. Because half of patients with very early active disease may not demonstrate correlation between the levels of IL-22 and disease activity20, this is important to note in this study.
On the other hand, contradictory data have been presented for correlation between IL-17 and disease activity. In line with 2 reports34,35 we observed that IL-17 levels did not correlate with DAS28 and CDAI findings. Higher IL-17 levels were recently associated with systemic measures of more active disease in 30 patients36; the small number of patients in the latter report must be taken into consideration and thus further study is needed.
A subset of CD4 T cells related specifically to the expression of IL-22 has been described that is distinct from Th17, Th1, and Th2 cells, and are termed Th22 cells. These cells express chemokine (CCR6) and skin-homing receptors (CCR4 and CCR10) and do not express interferon-γ (IFN-γ), IL-17A, or transcription factor related to the Th1 and Th17 T cell subsets37,38. The Th22 subset is induced by epidermic Langerhans cells and by plasmacytoid dendritic cells, and the inflammatory cytokine tumor necrosis factor-α and IL-6 are related to its expression37,39. Th22 cells might be important for skin homeostasis and in inflammation, because patients with psoriasis demonstrate increased Th22 cell populations40. Although the roles of Th22 cells in RA remain unclear, this subset of cells has been associated to RA and correlated with increased plasma levels of IL-22 in patients with RA30. Our analyses show that levels of IL-22 were significantly higher in our cohort of patients with RA, but not other cytokines expressed by other cell populations (Th1 and Th17) such as IFN-γ and IL-17 (data not shown). These observations indicate a possible pathogenic role of Th22 cells in RA.
Rheumatoid factor (RF) is the term for autoantibodies directed to the Fcγ chains of IgG molecules. IgM-RF can be detected in 60% to 80% of RA patients with established disease and can precede the onset of disease by several years. The physiologic role of RF is to enhance immune complex clearance. Immune complexes are also present in the joint. Therefore, RF may contribute to the activity and chronicity of RA through complement-mediated pathways. Further, the RF-producing B cells in synovial tissue of patients with RA may act as antigen-presenting cells and present (foreign or self) antigens to T cells through uptake of immune complexes. Thus, RF in serum and RF-producing B cells contribute to the pathophysiology of RA41. Our findings demonstrate a correlation between high levels of IL-22 and positive RF. In some animal models of RA, immune complex formation at joint tissues is a major element. In collagen-induced arthritis, IL-22 may regulate antibody production26, although B lymphocytes do not express IL-22RI13. Increased levels of IL-22 have been associated to RF in Sjögren’s syndrome24. Mature naive B cells become activated on meeting their cognate antigen and then participate in germinal center reactions, leading to a number of effector mechanisms including generation of plasma cells that secrete antibody41. The importance of Th17 cells in the mechanism by which IL-17 drives autoimmune responses by promoting the formation of spontaneous germinal centers in mice has been reported42. IL-17 is also associated with the survival and proliferation of human B cells and their differentiation into immunoglobulin-secreting cells43. Further, the importance of B lymphocytes in the regulation of Th17 response has recently been demonstrated. B lymphocyte depletion with rituximab, a monoclonal antibody directed toward the CD20 antigen on B lymphocytes, led to a reduction in the number of Th17 cells as well as decreased levels of IL-17A, IL-21, and IL-22 in patients with RA44. The association of autoantibodies and IL-22 requires further investigation. It is a limitation of our study that we did not investigate RF titers, CRP levels, extraarticular symptoms, and presence of anticyclic citrullinated peptides. It is widely accepted that there is an association of high-titer RF with more severe disease, thus we found significant correlation between high scores of DAS28 and CDAI and increased IL-22 levels. Most of our patients had longterm disease despite treatment, which may also indicate a more severe course of RA.
Although the findings were not statistically significant (p > 0.05), our in vitro results revealed a tendency to increased levels of IL-22 expressed by PBMC from patients with RA following stimulation. The results indicate a possible pathophysiological role of IL-22 in RA. The association of increased levels of this cytokine with disease activity in patients with established disease suggests the potential of IL-22 as an additional tool for assessment of activity in RA, particularly in patients with RF antibodies and longterm disease (mean 10.5 years). Taking into consideration that levels of IL-22 have been associated with bone erosions, this interleukin might be helpful in identifying patients with more destructive disease. Further studies are needed to clarify the role of IL-22 in RA.
Footnotes
-
Supported by the Fundação de Amparo à Ciência e Tecnologia do Estado de Pernambuco and Instituto Nacional de Ciência e Tecnologia para Inovação Farmacêutica (INCT_if).
- Accepted for publication March 30, 2012.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}