

Abstract
Objective. To investigate the mortality of hospitalized patients with systemic lupus erythematosus (SLE) and determine the influential factors associated with poor prognosis.
Methods. Medical records of 1956 SLE inpatients from 15 hospitals during the period January 1, 1999, to December 31, 2009, were reviewed. All patients were followed up in January 2010. Potential factors associated with mortality were analyzed, comparing patients who were living with those who were deceased. The independency of those factors significantly related to death was determined by Cox regression analysis.
Results. Male to female ratio was 1:15 in this cohort; median age at disease onset was 30 years. Hematologic (70.0%), mucocutaneous (68.2%), musculoskeletal (57.9%), and renal (48.7%) involvements were most often seen in these patients at time of admission. The overall mortality was 8.5% (n = 166), with infection (25.9%), renal failure (19.3%), and neuropsychiatric lupus (18.7%) the leading 3 causes of death. Independent predictors for mortality in this cohort of SLE patients were neuropsychiatric involvement [hazard ratio (HR) 2.19], anemia (HR 1.69), SLEDAI score > 8 at discharge (HR 1.64), increased serum creatinine (HR 1.57), low serum albumin (HR 1.56), cardiopulmonary involvement (HR 1.55), and patient untreated before admission (HR 1.48), whereas the use of antimalarial drugs (HR 0.62) and positive anti-Sm antibody (HR 0.60) were shown to be protective factors.
Conclusion. SLE patients with delayed treatment and refractory disease have poorer prognosis. A high incidence of death would be expected if they have neuropsychiatric involvement, anemia, azotemia, or cardiopulmonary involvement. Combination therapy with antimalarial drugs may provide some benefit to patients with SLE.
Systemic lupus erythematosus (SLE) is a chronic multisystem autoimmune disease predominantly affecting women of childbearing age. The disease is of great heterogeneity in that patients may possess pleiotropic manifestations and variable clinical courses. Although survival probability has improved significantly over the past several decades, to some extent SLE is still considered a fatal disease. Availability of prognostic information would allow better identification of patients at greatest risk of mortality and morbidity, who might then be candidates for more intensive monitoring and aggressive treatment.
Previous studies have displayed many predictors of poor disease outcome such as age of onset, sex, ethnicity, disease activity, renal disease, central nervous system lupus, anemia, and thrombocytopenia. However, there are disagreements among these studies, especially regarding the role of ethnicity, clinical manifestation, and disease activity, which could be partly explained by the improved morbidity and mortality due to better knowledge of disease pathogenesis, early diagnosis and treatment, and continuous development of new strategies to treat endstage organ failure.
There are few prognosis studies in Chinese patients with SLE as Chinese modern rheumatology started relatively late. To discern the most important predictors of survival in patients, we performed a multicenter study involving 15 hospitals in 9 cities under the supervision of the Jiangsu Rheumatology Association. Total data of more than 2000 patients with SLE hospitalized during the past 11 years were reviewed, and those with relatively complete information and available for contact by the end of January 30, 2010, were included.
MATERIALS AND METHODS
Patients
Medical records of SLE patients hospitalized from January 1, 1999, to December 31, 2009, in Jiangsu Province were reviewed. All patients fulfilled at least 4 of the revised and/or updated American College of Rheumatology criteria for classification of SLE1,2. Survival conditions of these patients were checked in January 2010 and those lost to followup were excluded from analysis. Patients with incomplete or loss of medical records were also excluded.
Data collection
A website was set up for the management of data from 15 hospitals (http://lupus.cinkate.com.cn:2222/). In total, 1956 SLE patients were enrolled (accounting for nearly 40% of total hospitalizations at these centers during the time interval 1999–2009), of which 1398, 202, and 74 had been hospitalized once, twice, and more than twice, respectively, while 282 patients had unknown previous hospitalization status. Information was obtained from patients’ ever recorded first admissions that included sex, age (at disease onset, diagnosis, and first hospitalization), initial manifestations, organ involvement, disease activity, concomitant diseases, family history, major laboratory results, and treatments. Organ involvement on admission was assessed according to the British Isles Lupus Assessment Group (BILAG) 2004 index3. Eight organ systems (mucocutaneous, musculoskeletal, neuropsychiatric, cardiopulmonary, renal, gastrointestinal, hematological, and ophthalmic) were retrospectively evaluated by experienced rheumatologists from 15 hospitals; patients were classified as having specific organ involvement if they had one of the manifestations. Disease activities on admission and at discharge were calculated according to the SLE Disease Activity Index (SLEDAI) score by chart review4. Normal values for laboratory tests in China were as follows: white blood cells 4–10 × 109/l, hemoglobin ≥ 110 g/l (female) or 120 g/l (male), platelets 100–300 × 109/l, alanine aminotransferase (ALT) < 60 IU/l, serum albumin ≥ 35 g/l, serum creatinine ≤ 133 μmol/l, antinuclear antibody (ANA)-negative (< 1:40), anti-dsDNA-negative, anti-Sm-negative. For patients who died before January 2010, ages and causes of death were documented.
Statistics
Data were analyzed by SPSS 16.0 software. Values were shown as number (percentage) or median (quartiles). Two-by-two tables were analyzed by chi-square or Fisher exact test as appropriate, whereas numeric data were analyzed by Mann-Whitney U test because most data had a skewed distribution. Factors significantly related to death in univariate analyses were entered into a Cox proportional hazards model (p value to enter < 0.05, p value to stay < 0.1) to determine their independency. Despite efforts to maximize data collection, some gaps remained (14.4% data missing for number of admissions, 17.7% missing for SLEDAI score at discharge, 0–5% missing for all other variables). Missing data were treated as normal values when performing regression analysis. Results were reported as hazard ratios (HR) with 95% confidence intervals (CI). Binary logistic regression analysis was applied to find clinical features associated with renal involvement, anti-Sm antibody, and treatment with antimalarial drugs, and results were reported as odds ratios (95% CI).
RESULTS
Summary of the cohort
Of 1956 patients with SLE, 1834 were female (male:female = 1:15). Median age at disease onset was 30 years (range 8–83 yrs). As shown in Figure 1, usual time of diagnosis of SLE was 1 year later (median 31 yrs, range 8–84 yrs). The median interval from disease onset to first hospitalization was 1.08 (0.17, 4.33) years (Table 1). More than half the patients had not been treated before and 1.7% had a positive family history; 16.5% had had multiple hospitalizations in the past 11 years.

Age distribution of the 1956 patients with SLE; case numbers shown for each year, with ages at disease onset, at diagnosis, and at first hospitalization. SLE is most common in the 20–40-year age group.
Characteristics of the Chinese SLE cohort. Data were retrieved through chart review of patient’s first hospitalization records except that the number of admissions was accumulated during the past 11 years (1999–2009). Total numbers might be less than 1956 because there were missing data in some subjects. All values are number (percentage) unless otherwise indicated.
At disease onset, malar rash and arthralgia/arthritis were the most common symptoms (40.6% and 38.7%, respectively) and few patients had renal involvement (6.3%), hematologic abnormality (4.6%), serositis (3.3%), and other features. The most common complaints for hospitalization were fever (30.8%), rash (28.8%), arthralgia (27.9%), edema (13.6%), and cough (10.2%). At time of admission, most patients were found to have hematologic (70.0%), mucocutaneous (68.2%), and musculoskeletal (57.9%) involvement (Table 1). Meanwhile, nearly half had kidney involvement, and renal biopsy was performed in only 90 cases, in which 11% had World Health Organization (WHO) class III, 48% WHO class IV, and 10% WHO class V results. About one-quarter of patients presented with cardiopulmonary manifestations, while neuropsychiatric involvement was noted in 6.3% (n = 122).
Laboratory tests showed that many patients had decreased white blood cells, hemoglobin, and platelets (44.5%, 42.8%, and 29.4%, respectively). More than half (n = 1042) had abnormal albumin levels and 8.3% (n = 154) had abnormal renal function. 94.0% of the patients were ANA-positive, antibodies to dsDNA were positive in 61.3%, and Sm antibodies were positive in 32.4%.
On admission, 75.7% of patients had a SLEDAI score > 8 and 27.2% had a score > 15. At the time of discharge, 30.4% of patients still had a SLEDAI score > 8 despite the treatment (Table 1).
Causes of death
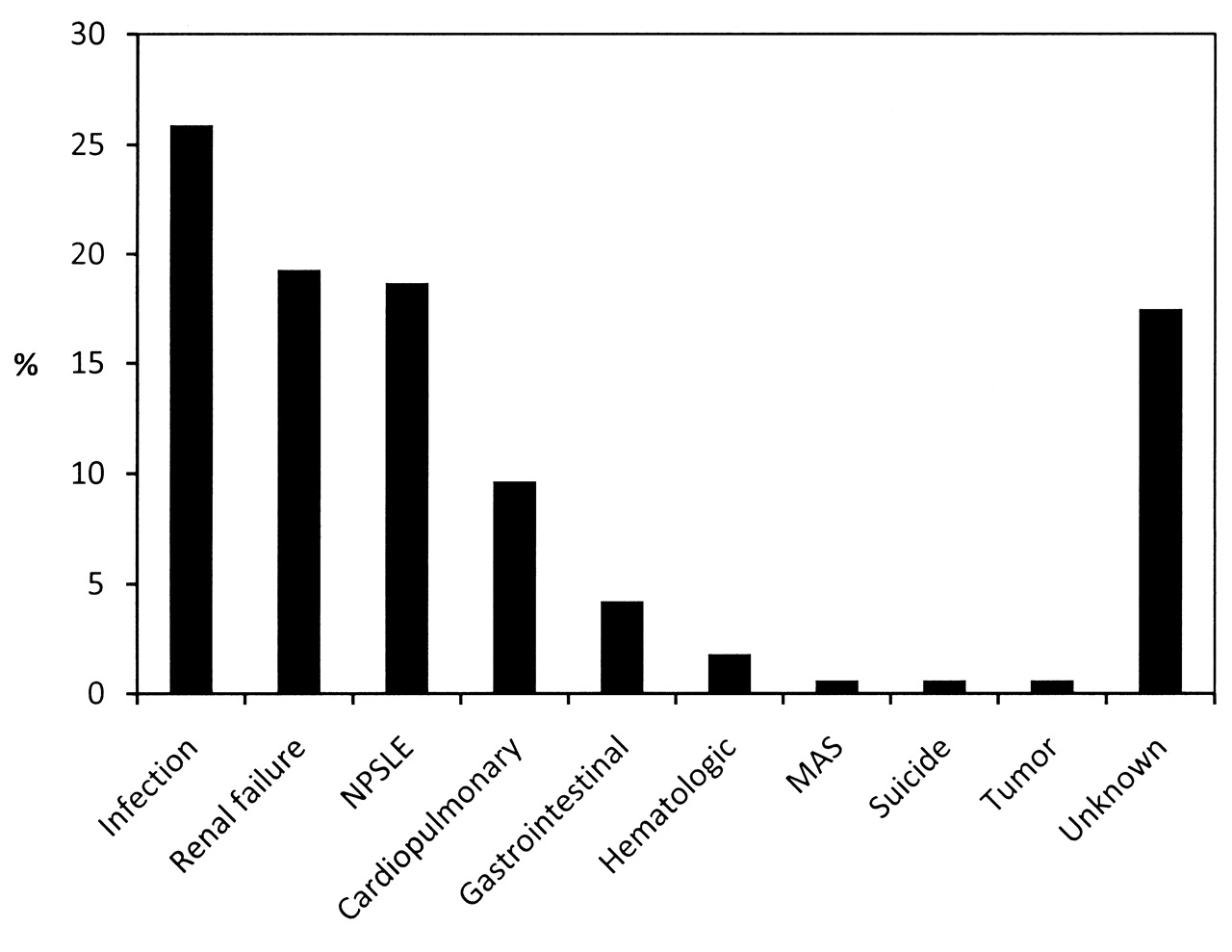
Overall mortality of this cohort was 8.5% (n = 166). The median age at death was 38 years (range 17–80 yrs). As shown in Figure 2, 3 main causes of death were infection (n = 43, 25.9%), renal failure (n = 32, 19.3%), and neuropsychiatric lupus (NPSLE; n = 31, 18.7%). SLE patients were most vulnerable to pulmonary infection, which caused 30 deaths (18.1%) in this cohort. 9.6% of patients died of severe cardiopulmonary involvement including interstitial lung disease (n = 6), pulmonary hypertension (n = 5), pulmonary hemorrhage (n = 1), myocardial infarction (n = 2), and sudden cardiac death (n = 2). Seven died of gastrointestinal complications including liver failure (n = 4), gastrointestinal bleeding (n = 2), and pancreatitis (n = 1). Other causes of death included hematologic involvement, macrophage activation syndrome, tumor, and suicide. Ill-defined causes of death, most recorded as cardiopulmonary failure or multiple organ failure, accounted for nearly 20% of the total deaths in the retrospective study and have been classified as unknown here.

Three main causes of death in our cohort were infection (n = 43), renal failure (n = 32), and neuropsychiatric lupus (NPSLE; n = 31). MAS: macrophage activation syndrome.
Among the 166 deaths, 103 occurred within 1 year after first admission (short-term mortality). Compared to those who died later, more deaths caused by NPSLE were seen in the early deaths (27 vs 4 cases, respectively; p < 0.01), while mortality caused by infection or renal failure was unchanged (32 vs 14 and 18 vs 14, respectively; all p > 0.05).
Factors associated with mortality
Various clinical and demographic factors were analyzed for their relationship with disease mortality. In a univariate model, factors associated with poor prognosis included male gender (p = 0.03), older age (age ≥ 40 yrs on admission; p = 0.04), longer time to hospitalization after onset (≥ 4.5 yrs; p = 0.001), untreated before admission (p < 0.001), more than one time of admission (p = 0.02), renal disease (p < 0.001), cardiopulmonary disease (p < 0.001), neuropsychiatric disease (p < 0.001), gastrointestinal involvement (p = 0.001), hematologic involvement (p = 0.002), ophthalmologic involvement (p = 0.008), high SLEDAI score on admission (> 15; p < 0.001) or at discharge (> 8; p < 0.001), anemia (p < 0.001), low platelet count (p < 0.001), high ALT (p = 0.02), low serum albumin (p < 0.001), and abnormal serum creatinine (p < 0.001). Meanwhile, musculoskeletal involvement (p = 0.01), positive anti-Sm antibody (p = 0.004), and antimalarial drug treatment (p < 0.001) were associated with benign outcome (Table 1).
Because there could be interactions among these factors, Cox regression was applied to determine the independency. The independent predictors for mortality in our cohort of SLE patients are shown in Table 2. Neuropsychiatric involvement [HR 2.19 (1.37, 3.50), p = 0.001], cardiopulmonary involvement [HR 1.55 (1.11, 2.17), p = 0.01], SLEDAI score > 8 at discharge [HR 1.64 (1.12, 2.42), p = 0.012], anemia [HR 1.69 (1.10, 2.59), p = 0.017], hypoproteinemia [HR 1.56 (1.05, 2.31), p = 0.028], increased serum creatinine [HR 1.57 (1.03, 2.40), p = 0.036], and untreated before admission [HR 1.48 (1.03, 2.12), p = 0.035] were significant risk factors for death; whereas positive anti-Sm antibody [HR 0.60 (0.41, 0.90), p = 0.012] and the use of antimalarial drugs [OR 0.62 (0.43, 0.88), p = 0.008] were protective factors.
Independent risk factors for mortality by Cox regression analysis.
To further confirm these predictors for mortality, patients with disease durations < 4 years were analyzed as an inception cohort. There were 106 deaths among 1465 patients in this cohort. As shown in Table 2, cardiopulmonary involvement [HR 1.57 (1.02, 2.40), p = 0.039], hypoproteinemia [HR 1.93 (1.19, 3.11), p = 0.007], and increased serum creatinine [HR 1.91 (1.08, 3.39), p = 0.027] were potential risk factors for mortality; while positive anti-Sm antibody [HR 0.52 (0.33, 0.84), p = 0.007] and the use of antimalarial drugs [HR 0.59 (0.39, 0.92), p = 0.019] remained to be protective factors.
Logistic regression analysis was performed to search for anti-Sm-associated clinical features, and no difference of organ involvement (especially renal, neurological, hematological, and cardiopulmonary) was observed between those with and those without anti-Sm antibody. However, patients with positive anti-Sm had a short time duration from disease onset to admission [OR 0.54 (0.41, 0.72), p < 0.001], a low incidence of being untreated prior to admission [OR 0.79 (0.63, 0.98), p = 0.03], and a high SLEDAI score at discharge [OR 1.56 (1.17, 2.08), p = 0.003].
Treatments and patient’s prognosis
Regarding the treatments for our cohort of patients, 98% took glucocorticoids, 45.5% took antimalarial drugs (n = 701 hydroxychloroquine; n = 189 chloroquine), and 52.7% received cyclophosphamide therapy or other immunosuppressives (Table 1). In our routine practice, glucocorticoids were administered to all patients except those with severe infections but only mild or no SLE activity. Antimalarial drugs were given to all patients, especially those with rashes, except patients with macular disease or heart block, while immunosuppressives were often given to patients with high disease activity and organ involvement. Antimalarials were the only kind of drug found to be associated with patient’s prognosis (Table 1 and 2). As shown in Table 3, patients taking glucocorticoids plus antimalarials had a significantly lower mortality rate, compared to those taking glucocorticoids alone (3.7% vs 12.7%, respectively; p < 0.001). Patients taking glucocorticoids plus antimalarial drugs and cyclophosphamide or other immunosuppressants, including azathioprine, cyclosporine, methotrexate, leflunomide, mycophenolate mofetil, or tripterygium (a Chinese medicine), also had a lower mortality rate compared to those taking only glucocorticoids and immunosuppressants (8.6% vs 10.9%; p < 0.01).
Association of drug treatments with patient’s outcome.
By logistic regression analysis, antimalarial drugs were independently associated with low incidences of neurological involvement [OR 0.61 (0.40, 0.92), p = 0.02], hypoalbuminemia [OR 0.79 (0.64, 0.97), p = 0.03], azotemia [OR 0.61 (0.42, 0.90), p = 0.01], and thrombocytopenia [OR 0.67 (0.53, 0.84), p < 0.001], but not the SLEDAI score at admission [OR 1.10 (0.84, 1.43), p = 0.49].
Factors associated with short-term mortality
To determine whether short-term mortality could be predicted by different risk factors, deaths that occurred 1 year later, after the first admission, were removed and data were reanalyzed by Cox regression. Similar to data shown above, neuropsychiatric involvement [HR 2.62 (1.51, 4.52), p = 0.001], anemia [HR 1.89 (1.10, 3.22), p = 0.02], high ALT [HR 1.89 (1.16, 3.08), p = 0.011], low platelets [HR 1.60 (1.02, 2.50), p = 0.042], low albumin [HR 1.75 (1.01, 3.05), p = 0.046], and SLEDAI score > 8 at discharge [HR 2.02 (1.27, 3.22), p = 0.003] were significant risk factors for mortality; whereas use of antimalarial drugs [HR 0.55 (0.34, 0.87), p = 0.011] remained beneficial. However, the presence of anti-Sm antibody was no longer a protective factor [OR 0.73 (0.46, 1.17), p = 0.19].
DISCUSSION
To our knowledge, this is the first large multicenter study in China evaluating the risk factors of hospitalized patients with SLE, a population considered to have severe disease. The overall mortality of our cohort was 8.5%, with infection being the most common cause of death, followed by renal failure and NPSLE. Our findings suggest that both vital organ involvement and treatment strategy could affect the outcome of SLE patients. Patients refractory to treatment (with a SLEDAI score > 8 at discharge) usually had a poor outcome, while antimalarial drugs had a protective effect for those patients.
The independent clinical manifestations that identified patients at increased risk of mortality were neuropsychiatric involvement, cardiopulmonary involvement, anemia, and abnormal serum creatinine, which confirms observations in several previous studies5,6,7. Renal involvement has been identified as an important predictor of survival in patients with SLE in some studies6,8,9,10,11. However, this factor was not independently associated with a poor outcome in our study. According to our data, risk factors for mortality for patients with renal involvement were male sex, neuropsychiatric involvement, cardiopulmonary involvement, anemia, and increased creatinine (data not shown), suggesting that only those with severe or refractory disease would have a poor prognosis. To support this premise, there is a study showing that 10-year patient survival is 95% for those patients with lupus nephritis who achieved complete remission, 76% for those achieving partial remission, but only 46% for those not attaining remission12. Meanwhile, evidence has shown that nephropathy and large amount of proteinuria are unrelated to survival, but creatinine levels do correlate inversely with outcome7,13.
It has been reported that men represent about 10% (range 4%–22%) of all SLE patients14,15. In this cohort, the male to female ratio was 1:15, which is slightly lower than expected. An explanation for this may be that early diagnosis for male patients might have been difficult 10 years ago, when a number of the study centers involved would have just been established. Several studies have shown that male gender in SLE is associated with poor outcome5,6,16,17. Our study demonstrated that men had higher rates of mortality than women (10.2% vs 5.9%, respectively), but this observation had a lack of independency. Meanwhile, male patients may have more vital organ involvement and higher disease activity, which could be attributed in part to their later diagnosis.
Consistent with previous reports5,13, ANA and anti-dsDNA were not associated with survival. Interestingly, our data show that anti-Sm antibody was an independent protective factor for SLE, and those patients with positive anti-Sm were more likely to survive. There is still some debate on the relationship between anti-Sm/RNP and clinical manifestations as well as disease mortality18,19. In a recent study, the presence of anti-Sm antibodies was associated with arthritis, renal involvement, malar rash, and vasculitis20. There was no association between anti-Sm and organ involvement in our cohort, but anti-Sm is closely connected to a short duration from onset of disease to admission and a high disease activity at first discharge. To our knowledge, patients with positive anti-Sm, a specific antibody for diagnosis of SLE, can be identified early and thus promptly treated. These patients may not benefit in a short-term period because they usually have severe disease. But if the observation time is longer, their mortality risk is reduced.
Our analyses show that antimalarials are the only class of drugs that exerted a clear protective effect on survival. The benefit of antimalarials has been reported by several studies21,22,23. These drugs, among which hydroxychloroquine has been widely investigated, have been shown to possess immunoregulatory properties and mild anticoagulant properties, and also have a favorable effect on serum lipid profile and glucose concentrations21,24,25,26. Thus, by preventing the formation of autoantibodies and immune complexes, decreasing the occurrence of vascular thrombotic events, and maintaining a normal physiological metabolism, antimalarials may have a unique therapeutic profile for patients with SLE. Based on our data, a low incidence of neurological involvement, renal failure, and thrombocytopenia would be expected from therapy with antimalarials.
There was no survival benefit from other immunosuppressants, including cyclophosphamide. As with glucocorticoids, these drugs could have contradictory effects for SLE patients. Their potent effects help control severe disease; on the other hand, serious side effects could emerge using these drugs, especially infections, which are still the most common cause of death in China and other emerging countries10,27. In a large cohort study of Chinese patients with SLE, use of cyclophosphamide was identified as a risk factor for death, reminding us that more judicious use of immunosuppressive treatment should be considered to minimize infectious complication22.
There are some shortcomings in this study. First, socioeconomic status, a known predictor of poor survival in SLE5, was not evaluated. In routine practice, we find that in general patients without medical insurance or those from rural areas have a delay to proper diagnosis and treatment, which is likely to contribute to poor outcome. Second, data on treatment were limited to those obtained during the hospitalization. After patients are discharged, the chances they continue taking glucocorticoids, antimalarial drugs, and immunosuppressives are 97%, 75%, and 50%, respectively, within 1 year. A followup of treatment changes would be helpful to elucidate the role of immunosuppressants in mortality. Third, only hospitalized patients with SLE were included in this cohort, which means that all the conclusions were conditional on having sufficiently severe SLE. Moreover, potential bias may be introduced, as patients’ profiles among the study centers were quite different. Evidence has shown that patients have lower risks of mortality if hospitalized at medical centers with staff that are highly experienced28. A continued followup of our patients is under way. Accompanied by rapid development of the field of rheumatology in China, we expect a better prognosis for patients with SLE in the future.
Acknowledgment
The authors thank all investigators who participated in this study, and Dr. Ornella Rullo for help in the preparation of this report.
Footnotes
-
This study was partly supported by grants from Cinkate Pharmaceutical Company.
- Accepted for publication February 16, 2011.








{kind=link}
{kind=link}